Introduction
Uterine carcinosarcomas, known as malignant mixed mullerian tumors (MMMT) show characteristics of both carcinomas and sarcomas. According to Western studies, uterine carcinosarcomas constitute less than 5% of all uterine malignancies and about a half of all uterine sarcomas [1]. It is also known to frequently occur in postmenopausal women, especially in those who have received pelvic radiation therapy [2,3].
Uterine carcinosarcomas were conventionally considered as a subtype of uterine sarcomas. Therefore, the same treatment as the one used for treating uterine leiomyosarcomas and undifferentiated endometrial carcinomas was used. However, unlike the uterine leiomyosarcomas, the uterine carcinosarcomas exhibit more isolated local recurrences or lymph node metastasis rather than distant failure, which is similar to the failure pattern in uterine carcinomas [4]. Several pathological clues were found that support the idea that uterine carcinosarcomas can be categorized as a type of metaplastic carcinoma, since they are monoclonal in origin [5,6]. Based on such findings, in 2009, the revised International Federation of Gynecology and Obstetrics (FIGO) staging system classified uterine carcinosarcoma separately from sarcoma and put it under the category of carcinoma [7]. Also, the current treatment guideline recommends treating uterine carcinosarcoma according to the guideline of high grade carcinoma [8]. Uterine carcinosarcoma tends to show poor prognosis compared to the high grade carcinoma, because it is diagnosed at the advanced stage and is also aggressive in nature [9,10].
Uterine carcinosarcomas are rare. Thus, it is difficult to come up with a reliable treatment policy based on results from randomized clinical trials. Currently there is no consensus with regard to the optimal adjuvant treatment of the uterine carcinosarcomas due to the fact that many retrospective studies were conducted with a small number of patients using various different treatment methods. However, the radiation therapy is considered potentially effective to reduce the recurrence rate in pelvic and para-aortic lymph nodes, because failures occur in these areas. Moreover, according to recent studies in uterine malignancies, postoperative radiation therapy (PORT) was reported to significantly reduce the local recurrence of tumors in such population [11,12].
The goal of this study was to evaluate the effects of PORT on patterns of failure and survivals in uterine carcinosarcoma patients, who received radical surgery at Seoul National University Hospital.
Materials and Methods
1. Patients
A total of 19 patients were diagnosed as uternie carcinosarcoma after radical hysterectomy at Seoul National University Hospital between October 1998 and August 2010. Patients whose cancer was metastasized were excluded in the study even if they had hysterectomies. Among the 19 patients, 11 received PORT and the other 8 did not. The analysis was done retrospectively by reviewing patients' medical history and examination results.
The age distribution of the patients was from 33 to 78 years (median, 60 years). Sixteen patients were menopausal status at the time of diagnosis. Two patients had previous pelvic irradiation history, and one of them had radical radiotherapy for cervical cancer 25 years before she was diagnosed as uterine carcinosarcoma. The other patient had PORT after rectal cancer surgery 12 years before her diagnosis.
Physical examination, blood test, chest X-ray, chest computed tomography (CT), and intravenous pyelography were conducted for the preoperative staging. Thirteen, 11, and 7 patients received pelvic magnetic resonance imaging (MRI), positron emission tomography (PET)-CT, and pelvic CT respectively. Pap smear test results were available in 16 patients.
2. Surgery and staging work-up
All 19 patients received hysterectomy and bilateral salpingo-oophorectomy. They also had pelvic lymph nodes dissection except for 2 patients whose lymph nodes were sampled for biopsy. Among 9 patients who additionally received para-aortic lymph node sampling, one patient reported as having metastatic lymphadenopathy on frozen section examination had para-aortic lymph node dissection. The results of peritoneal washing cytology were available in 16 patients.
3. Radiotherapy
Postoperative radiotherapy was carried out on the radiation oncologists' discretion. Among the 19 patients, 11 (57.9%) had the whole pelvis radiotherapy (WPRT), but no brachytherapy was done. External beam radiotherapy was delivered with 6-16 MV photon beams using 4 portals in daily fractions of 1.8 Gy. The borders of pelvic portal were as follows: superior, L4-5 interspace; inferior, obturator foramen; lateral, 1.5 cm lateral to pelvic brim; anterior, anterior to symphysis pubis; posterior, S2-3 interspace. For 9 patients who received the treatment after 2006, 3-dimensional conformal radiation therapy (3D-CRT) based on CT was carried out. The intended radiation dose for WPRT was 50.4 Gy, however, one patient missed a treatment and received 48.6 Gy. A patient proved to have para-aortic lymphadenopathy was irradiated with 45 Gy to para-aortic lymph nodes region.
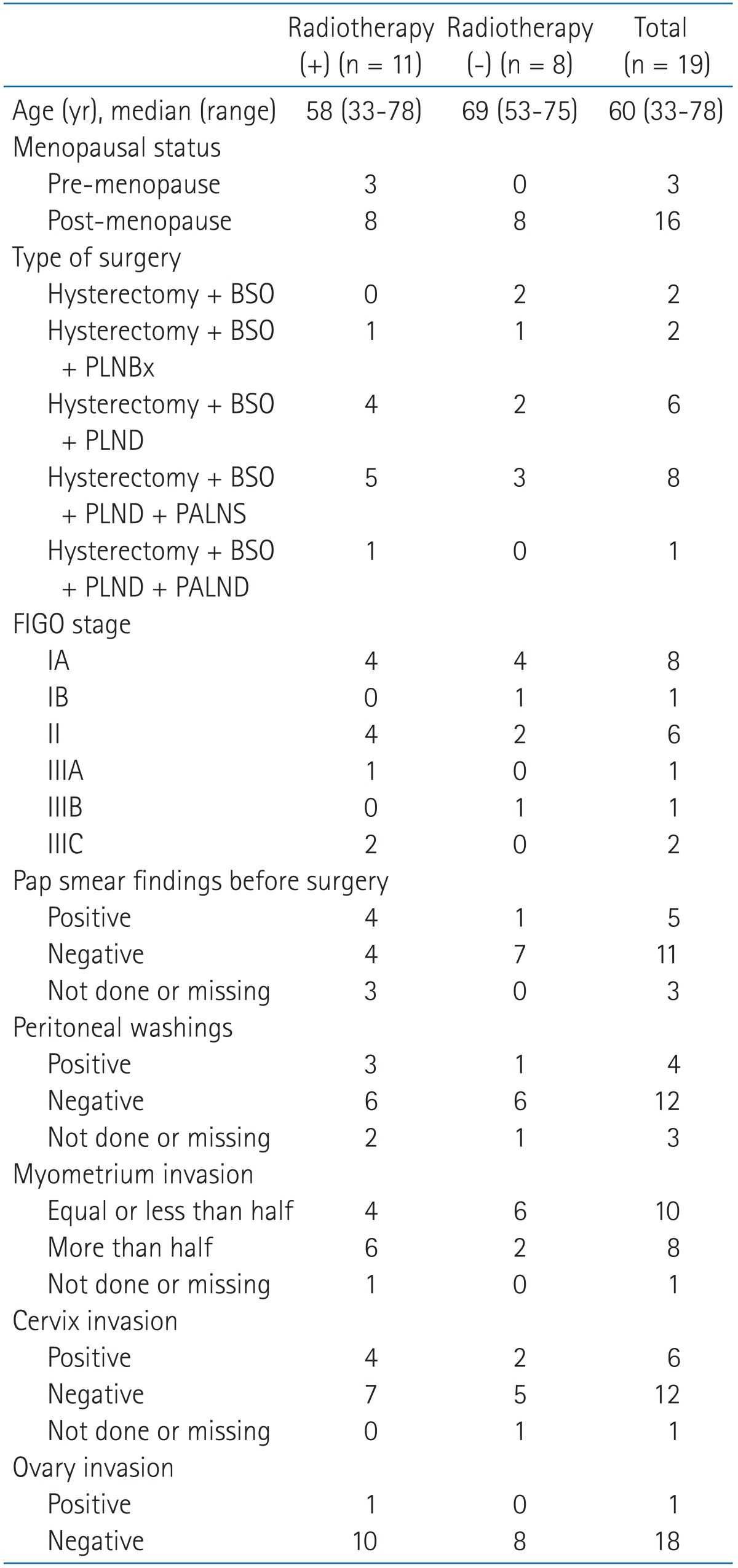
The summary of the characteristics of patients and tumors according to the radiation therapy is shown in Table 1.
4. Chemotherapy
Among the 11 patients who received PORT, 6 patients had concurrent chemotherapy. Three patients had paclitaxel and carboplatin. One had doxorubicin and cisplatin, the other one had ifosfamide and cisplatin. The remaining one patient received clisplatin alone. No patient received adjuvant chemotherapy after completion of radiotherapy. Three patients had salvage or palliative chemotherapy after recurrence.
Among the 8 patients who did not receive PORT, 3 received adjuvant chemotherapy after surgery. Salvage chemotherapy was carried out for 2 patients whose cancer had recurred. Two patients who had previous WPRT did not have PORT.
5. Recurrence evaluation
After the completion of radiotherapy, patients were closely monitored every 3 months during the first 2 years, every 3 months during the next 2 years, and every 6 months during the next 5 years. After that, patients received annual physical examination with blood test and imaging study. Local recurrence was defined as recurrence at the vagina or at the tissues in the vicinity of the vagina. Regional recurrence was defined as tumor recurrence at pelvic or para-aortic lymph nodes according to the 7th edition of American Joint Committee on Cancer (AJCC) cancer staging. Distant metastasis was defined as treatment failure at any other location except previously mentioned area. For recurrences that were diagnosed by histologic or cytologic exams, the test date was used as the failure date of the treatment. For recurrences that were diagnosed by imaging study, the failure date of the treatment was set as the date when the MRI or CT was taken.
6. Statistical analysis
SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA) was used for the statistical analysis. The Kaplan-Meir method was used in order to obtain the graph for the life expectancy and the survival rate of the patients. The differences in the survival rate were estimated using the long-rank test. A p-value < 0.05 was used to determine the statistical significance for all tests.
Results
1. Patterns of failure
The follow-up duration from the date of first treatment varied from 7.8 to 126.6 months (median, 22.7 months). Seven patients (36.8%) showed treatment failures. Four patients (36.4%) experienced recurrence in PORT group, whereas 3 patients (37.5%) had recurrence in non-PORT group (p = 0.922).
All 4 treatment failures from PORT group were distant metastasis and 2 of them also had regional recurrences. Two patients who had lymph node metastasis upon diagnosis experienced regional recurrences despite radiation treatment. One of the patients showed distant metastasis followed by para-arotic lymph node metastasis and the other patient revealed distant metastasis and regional recurrence at pelvic and para-arotic lymph nodes simultaneously. On the other hand, 3 treatment failures in non-PORT group were all loco-regional recurrences. Among them, one patient developed distant metastasis simultaneously (Table 2).
The treatments and the recurrence patterns of the patients who showed treatment failures are summarized in Table 3 according to their stage. Among these patients, patients who received PORT also had concurrent chemotherapy, but they did not receive the additional adjuvant chemotherapy unless it was evident that tumor recurred. A stage IIIB patient with previous WPRT history due to rectal cancer did not receive PORT. Instead she had adjuvant chemotherapy. After the treatment failure, 5 out of 7 patients received salvage chemotherapy. Three patients who did not have PORT did not receive radiation therapy (RT) for salvage purpose. By the time the results were analyzed, all patients who had failed died except one. The only survived patient had local recurrence without distant metastasis and she is alive with disease. All treatment failures occurred within 12 months from the date of surgery.
2. Survivals and prognostic variables
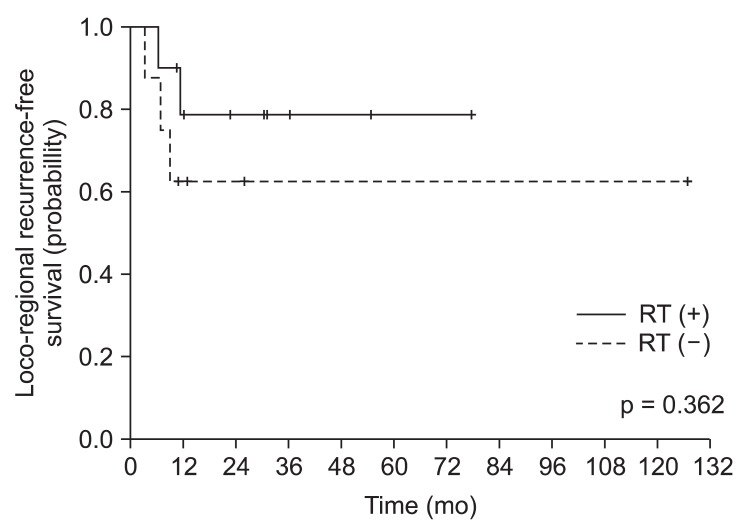
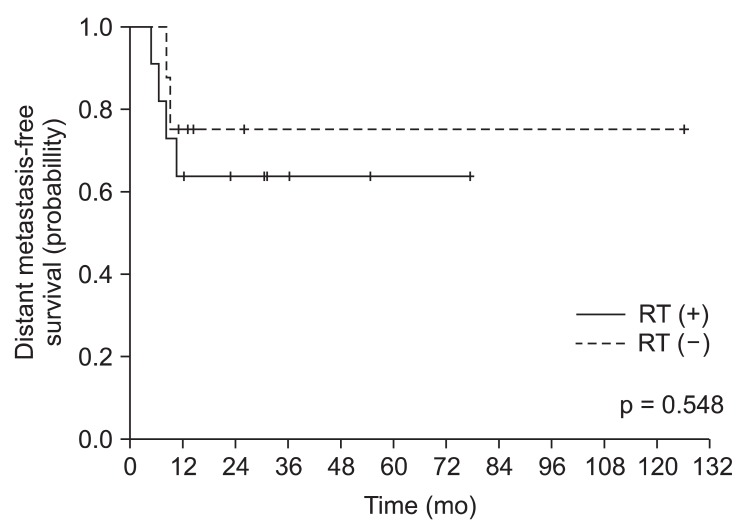
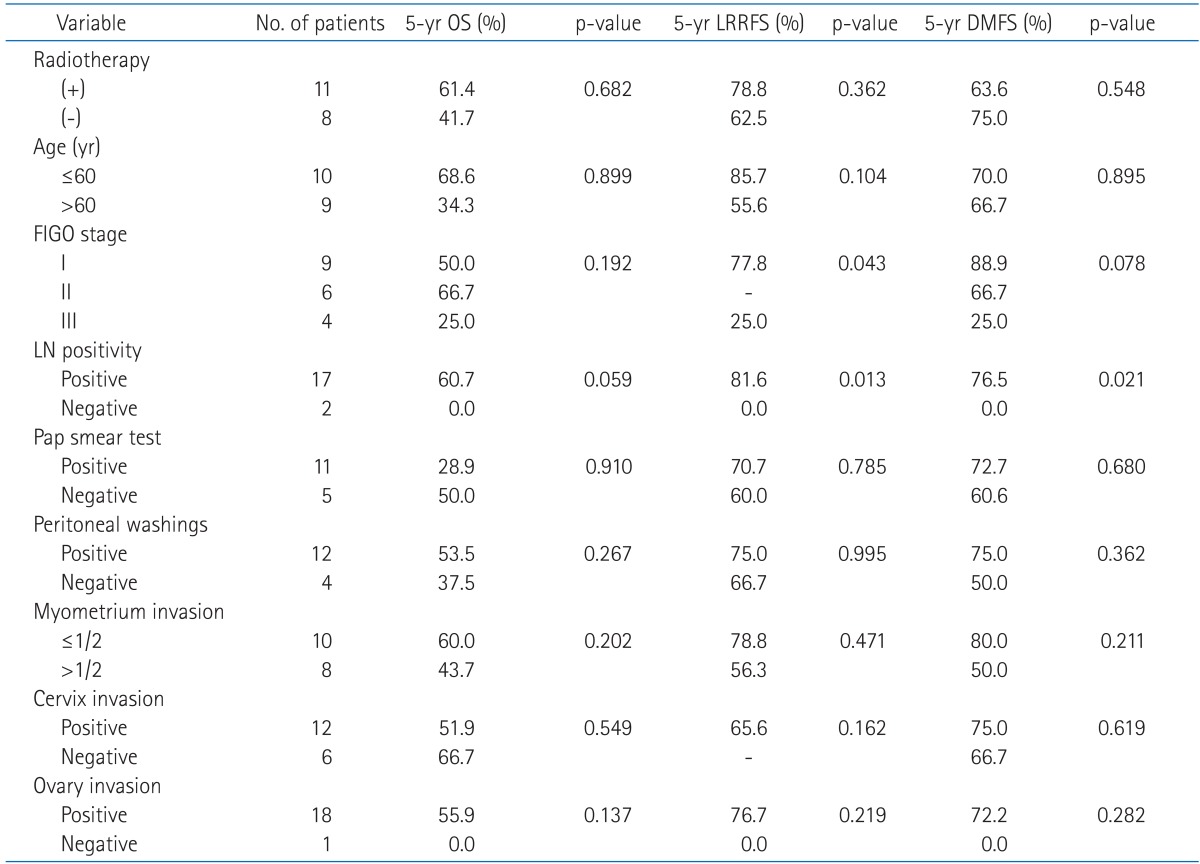
The 5-year overall survival rate (OS) was 51.9% for all patients, 61.4% in PORT group, and 41.7% in non-PORT group, respectively. There was no statistical difference between the two groups (p = 0.682) (Table 4). The predominant failure was distant metastasis in PORT group, but that was local recurrence in non-PORT group. Despite this difference between the two groups, the 5-year loco-regional recurrence free survival rates (LRRFS) were 78.8% and 62.5%, respectively (p = 0.362), and 5-year distant metastasis free survival rates (DMFS) was 63.6% and 75.0%, respectively (p = 0.548), with no statistically significant difference (Figs. 1 and 2).
The results of the univariate analysis of variables such as PORT, age, FIGO stage, preoperative pap smear test, peritoneal washing cytology, myometrium invasion, cervix invasion, and ovary invasion are shown in Table 4. Two patients who were diagnosed with lymph node metastasis had low LRRFS (p = 0.013) and DMFS (p = 0.021), which were statistically significant. When the result was analyzed according to FIGO staging system, the higher the disease stage, the lower the LRRFS was as well as the DMFS was. Positive result of peritoneal washing cytology, which was considered as stage III before the revision of FIGO stage, did affect neither loco-regional recurrence nor survival rates.
3. Treatment toxicity
There was no complication higher than grade 3 associated with the treatment according to Common Terminology Criteria for Adverse Events (CTCAE) v3.0 [13]. However, there were two cases of grade 1-2 lymphedema of lower extremity in PORT group and one case of grade 2 lymphocele in non-PORT group.
Discussion and Conclusion
Uterine carcinosarcoma, which used to be considered as a type of sarcoma in the past, is now being classified as metaplastic carcinoma. In general, the prognosis of this entity is poor compared to high-risk endometrial cancer. According to recent studies, the 5-year survival rate of the uterine carcinosarcoma patients is approximately 30-50% [3,11,14]. In our study, the 5-year survival rate of all patients was 51.9%, which was equivalent or a bit higher compared to the results from other studies. Our study also showed that all seven cases of the first treatment failure occurred within 12 months from the date of surgery. This result is similar to the studies reported by Sartori et al. [15] and Wolfson et al. [16], in which treatment failure tended to happen early.
The main treatment for uterine carcinosarcoma is surgery, which includes hysterectomy and bilateral salpingo-oophorectomy with or without pelvic lymph node dissection selectively. In addition, peritoneal washing cytology is performed along with biopsy of the suspicious regions, and omentectomy is also carried out at the physician's discretion. However, no consensus has been established regarding the optimal postoperative adjuvant therapy.
Reed et al. [12] reported the results of subgroup analysis of uterine carcinosarcoma from their phase III clinical trial. This study randomly assigned stage I-II uterine carcinosarcoma patients to the PORT or the observation groups after surgery. It allowed the selective performance of pelvic and para-aortic lymph nodes dissection, and the lymph node sampling was carried out in approximately a quarter of the patient pool. The PORT for the carcinosarcoma group significantly reduced the local recurrence, which was different from the leiomyosarcoma group. However, this reduction of local recurrence did not result in improving the disease free or overall survival rate. In addition, the recent large scale retrospective study done by Sampath et al. [11], who analyzed 1,877 uterine carcinosarcoma patients, reported that the PORT significantly increased LRRFS (5 years, 84% vs. 95%, p < 0.001). Furthermore, Callister et al. [3] reported that pre- or postoperative radiation therapy not only improved the pelvic disease control rate (5 years, 52% vs. 72%, p = 0.0001), but also affected the increased OS rate (5 years, 27% vs. 36%, p = 0.069).
Most studies previously described indicated that PORT reduces the loco-regional recurrence, but does not improve OS. However, several studies reported that adjuvant radiation therapy did increase the OS. According to the analysis of Clayton Smith et al. [17] using Surveillance Epidemiology, and End Results (SEER) data, 890 out of 2,461 patients received PORT and the OS increased from 33.2% to 41.5% (p < 0.001) with the addition of PORT. When the data from stage I-III patients were analyzed, there was also a statistically significant improvement in the OS (p = 0.03).
Our study did not demonstrate that PORT provided the treatment benefit in terms of improving LRRFS, DMFS, and OS. However, except for the two patients who had lymph node metastasis at diagnosis, there was no loco-regional recurrence among patients who had PORT. There were 3 local recurrences among patients who did not receive PORT. Therefore, it can be inferred that PORT for uterine carcinosarcoma patients was effective as a local therapy to prevent loco-regional recurrence even though it is difficult to make any statistical significance due to the small size patient pool. Also, the role of adjuvant systemic chemotherapy can be inferred in that 6 out of 7 failure cases had distant metastasis and PORT reduced loco-regional recurrences.
In this context, there have been several studies which have investigated the role of adjuvant therapy in uterine carcinosarcoma using multimodal approach since year 2000 [18-20]. These studies all show that treatment, which includes surgical operation, radiation therapy, and chemotherapy, increased the OS of uterine carcinosarcoma patients compared to treatment that only involves PORT or chemotherapy alone. In the case of our study, concurrent chemotherapy was applied to 6 patients among 11 who received PORT, but none of them had additional chemotherapy.
It is well known that the stage is a powerful prognostic factor. However, with regard to the other prognosis variables, different results have been reported depending on researchers. Yamada et al. [21] reported that more than half of myometrium infiltration, lympho-vascular space invasion, positive result of peritoneal washing cytology, adnexa invasion, uterine serosa invasion, and lymph node metastasis were factors that contributed to poor prognosis in terms of disease free interval. The adjuvant radiation therapy was related to the increased OS (p = 0.03). Callister et al. [3] reported that postmenopausal status at diagnosis, uterus length more than 10 cm, and cervix invasion were factors that contributed to poor cause specific survival rate. The study also showed that peritoneum infiltration, previous history of pelvic radiation therapy, and not receiving radiotherapy were independent factors that contributed to poor pelvic control rate [3]. Our study showed that the stage was the prognostic factor for LRRFS (p = 0.043), but it marginally affected the DMFS (p = 0.078). Among the factors mentioned previously, lymph node metastasis was the only factor that affected both LRRFS (p = 0.013) and DMFS (p = 0.021) with statistical significance. It also affected the OS (p = 0.059). However, it is difficult to make any definitive conclusion due to the small number of patients. Thus, additional studies need to be done with a larger number of patients in the future.
In conclusion, the 5-year OS of the uterine carcinosarcoma patients who were treated at Seoul National University Hospital was 51.9%, and the 5-year LRRFS was 78.8% in PORT group. Although our results did not show any statistical significance because of the small number of patients and limited follow-up period, PORT can be considered as effective in preventing loco-regional recurrence based on the patterns of treatment failure. Considering that most treatment failures were distant metastasis, a multi-modal treatment approach that combines surgery, adjuvant radiotherapy, and chemotherapy for uterine carcinosarcoma should be considered.