Introduction
Nasopharyngeal carcinoma (NPC) shows markedly geographic and racial variations in incidence. South Korea is known to show an intermediate incidence, which is lower than that of an endemic area and higher than that of the Western world. According to the most recent annual report of cancer statistics in South Korea, NPC accounted for 0.2% of all malignancies [1]. NPC has a tendency of early lymphatic spread and a higher incidence of cervical lymph node metastasis among head and neck cancers [2]. Because of the risk of lymph node metastasis, the fields of radiotherapy (RT) for NPC traditionally encompass the primary disease and involved neck nodes, as well as the entire draining lymphatic regions to the lower neck.
Advances in imaging technology have substantially improved the ability to detect nodal metastases and knowledge about the patterns of lymphatic spread. The study by Tang et al. [3], which was based on magnetic resonance imaging (MRI), showed that only 0.3% of patients without the first station lymph node showed spread to level IV or supraclavicular lymph nodes, skipping the second station. A meta-analysis of 2,920 patients from 13 studies using MRI as the main imaging modality by Ho et al. [4] showed that nodal metastases followed an orderly pattern and the probability of skip metastasis between levels varied between 0.5% and 7.9%. According to these results, the rarity of skip metastasis in NPC lymphatic drainage provides a basis to eliminate irradiation of the entire cervical lymph nodes, and only encompass the echelon inferior to the involved level.
Furthermore, treatment of a large field to the neck is associated with substantial morbidities, both early and late. Acute toxicities include mucositis and dermatitis, especially if concurrent chemo-radiation is utilized; late toxicities may include xerostomia, neck fibrosis, lymphedema, cranial neuropathy, endocrine dysfunction, trismus, eyeball damage, and deafness [5]. If selective neck irradiation can be safely implemented in patients with limited nodal disease burden, selective neck irradiation may improve the tolerability of RT, as well as patient compliance and quality of life. The introduction of intensity modulated RT (IMRT) has a more favorable balance between target coverage and the sparing of adjacent organs at risk. In South Korea, the RT techniques for NPC have been advanced remarkably to adopt the IMRT technique [6].
Since 2006, our institution's approaches have been geared towards reducing the lower neck fields or selecting treatment of the neck lymph nodes during the treatment of NPC. The aim of this report is to study the clinical outcomes and patterns of failure after RT with individually tailored fields of elective neck nodal irradiation for NPC at a single institution.
Materials and Methods
1. Patients and pretreatment evaluation
All patient cases with histologically approved NPC who received definitive aimed RT between September 2006 and May 2013 at Kyungpook National University Hospital were retrospectively reviewed. Since September 2006, 70 NPC patients without evidence of distant metastasis were treated with a reduced volume approach for elective nodal irradiation (ENI). Fourteen patients were excluded due to incompletion of planned treatment, insufficient evaluation for response, follow-up lost and follow-up of fewer than 3 months. Fifty-six patients were eligible for this analysis. Stage and treatment information for each patient was then obtained.
All patients underwent a complete medical history interview and physical examination, nasopharyngoscopy, ultrasonographic evaluation of neck nodes, computed tomography (CT) of the head and neck, and positron emission tomography/computed tomography (PET/CT). In selected patients who were suspected of skull base involvement, we performed an MRI of the skull base.
Because the initial diagnosis and treatment for this study's patients began in September 2006, patients were initially staged according to the 2002 American Joint Committee on Cancer (AJCC) system (6th edition). After the publication of the 2010 AJCC system, all patients were restaged using the new system (7th edition). All patients with positive lymph nodes in the cervical region were distinguished according to the criteria described by van den Brekel et al. [7] (i.e., shortest axis of Ōēź11 mm in the jugulodigastric regions, or >10 mm in other cervical regions).
2. Radiotherapy
We treated patients with NPC by delivering either moderate hypofractionation scheduled IMRT or conventional fractionation scheduled three-dimensional conformal radiotherapy (3D-CRT). IMRT was delivered to 38 patients and 3D-CRT was delivered to 18 patients. The median overall treatment time of RT was 57 days (range, 44 to 71 days). All patients were immobilized in the supine position with a thermoplastic mask. After administration of intravenous contrast material, 3-mm CT slices were acquired from the vertex to the carina. All target volumes were delineated slice-by-slice on the treatment planning CT scan.
The gross target volume (GTV) was defined as the gross tumor and involved regional nodes, which were defined by CT and PET/CT scans in all patients. The clinical target volumes (CTV) were individually delineated on the basis of tumor invasion patterns. High-risk subclinical disease (CTV-1) was defined as the GTV plus 1ŌĆō5 mm margin for high-risk microscopic extensions including the entire nasopharynx, both retropharyngeal nodes (RPNs) and the level of involved nodes. The low-risk subclinical area (CTV-2) was defined by adding 2ŌĆō5 mm margin to CTV-1 and the next neck level of CTV-1 areas based on tumor location and size, at the discretion of the radiation oncologist. Each CTV was expended to the planning target volume (PTV). The PTV1 was defined by adding a 3ŌĆō5 mm margin to the GTV, dependent on the GTV proximity to critical structures (e.g., brainstem, spinal cord, parotid gland, or brachial plexus). A 3ŌĆō5 mm margin was used for expansion to CTV-1 and CTV-2. PTV2 (CTV-1 + 3ŌĆō5 mm margin) covered areas considered at high risk for potential microscopic disease. PTV3 (CTV-2 + 3ŌĆō5 mm margin) included the clinically negative cervical lymphatic pathway.
In IMRT planning, we used a simultaneously integrated boost IMRT technique. The moderate hypofractionation scheduled IMRT delivered 72.6 Gy at 2.2 Gy per fraction to PTV1, 66 Gy at 2.0 Gy per fraction to PTV2, and 49.5 Gy at 1.5 Gy per fraction to PTV3. The conventional fractionation scheduled 3D-CRT delivered a total dose of 68.4ŌĆō72 Gy (median, 72 Gy) at 1.8ŌĆō2.0 Gy per fraction to the PTV1 and PTV2 with a reduced dose (median, 39.6 Gy; range, 39.6 to 45 Gy) to the PTV3 (elective neck lymphatics).
ENI always included the uninvolved levels II, III, and Va, but omitted level Ib, IV, and Vb nodes depending on involved lymph node location. The level Ia and level VI nodal areas were not irradiated in all patients. The level Ib was not routinely included for ENI, unless an involved node in level Ib was observed on imaging. In ENI for lower neck, the next station nodal area of the involved lymph node level was included in the volume for ENI, and not the more distal parts. More specially, the patient with enlarged level II lymph nodes was prophylactically irradiated to the level III nodal area, and was not irradiated to lymph node area of level IV, Vb, and supraclavicular area. In case of patients with only unilateral lymph node involvement (N1 disease), ENI of the ipsilateral neck included the next nodal station of the involved nodal area, and ENI of the uninvolved contralateral neck included only the level II, III, and Va nodal areas (Fig. 1).
3. Chemotherapy
Concurrent chemoradiotherapy (CCRT) using capecitabine and cisplatin (XP) or cisplatin alone for 2 to 3 cycles was used in all patients. In addition, 32 patients with advanced tumor disease or advanced neck nodal disease also received neoadjuvant or adjuvant chemotherapy. Chemotherapy was not administered uniformly to all patients according to any single protocol but was instead used at the discretion of the attending physician in individual cases.
4. Follow-up
Each patient was assessed at regular intervals for treatment response and toxicity both during and after RT. During RT, patients were evaluated once per week. At the end of treatment, patients were followed up 1 month after RT and every 3 months during the first and second years and every 6 months during the next 3 years, then once every year afterwards. Endoscopy and PET/CT were performed for all patients about 2ŌĆō3 months after the completion of treatment. During the follow-up session, CT to the head and neck region, PET/CT, and a physical examination were performed. When locoregional recurrences were suspected in endoscopy, CT, MRI or PET/CT, biopsies were performed for confirmation.
5. Definition of failure site
For patients with locoregional failure, the image scans of recurrent tumors were transferred to the pretreatment planning CT. The exact site and extent of each tumor was then compared with the pretreatment planning CT data sets, focusing on the 95% isodose lines of the prescription dose. Failures were categorized according to the criteria described by Dawson et al. [8] as occurring inside or outside the previously irradiated targets, depending on the location of Vfail: 'in field' if 95% of Vfail was within the 95% isodose, 'marginal' if 20% to 95% of Vfail was within the 95% isodose, or 'outside' if less than 20% of Vfail was inside the 95% isodose.
6. Endpoints and statistical methods
The follow-up period was measured from the date of completion of RT to the date of death, date of telephone survey or date of the last clinic visit before analysis. The primary endpoint was the relapse rate within the unirradiated nodal areas. Secondary endpoints included patterns of nodal relapse, locoregional control (LRC), distant failure-free (DFF), overall survival (OS), and disease-free survival (DFS). The rates of LRC, DFF, OS, and DFS were estimated using the Kaplan-Meier method. The differences were compared with the log-rank test. All statistical tests were two-sided, and p-values of Ōēż 0.05 were considered significant. All statistical analysis was performed using SPSS ver. 19.0 (IBM, Armonk, NY, USA).
Results
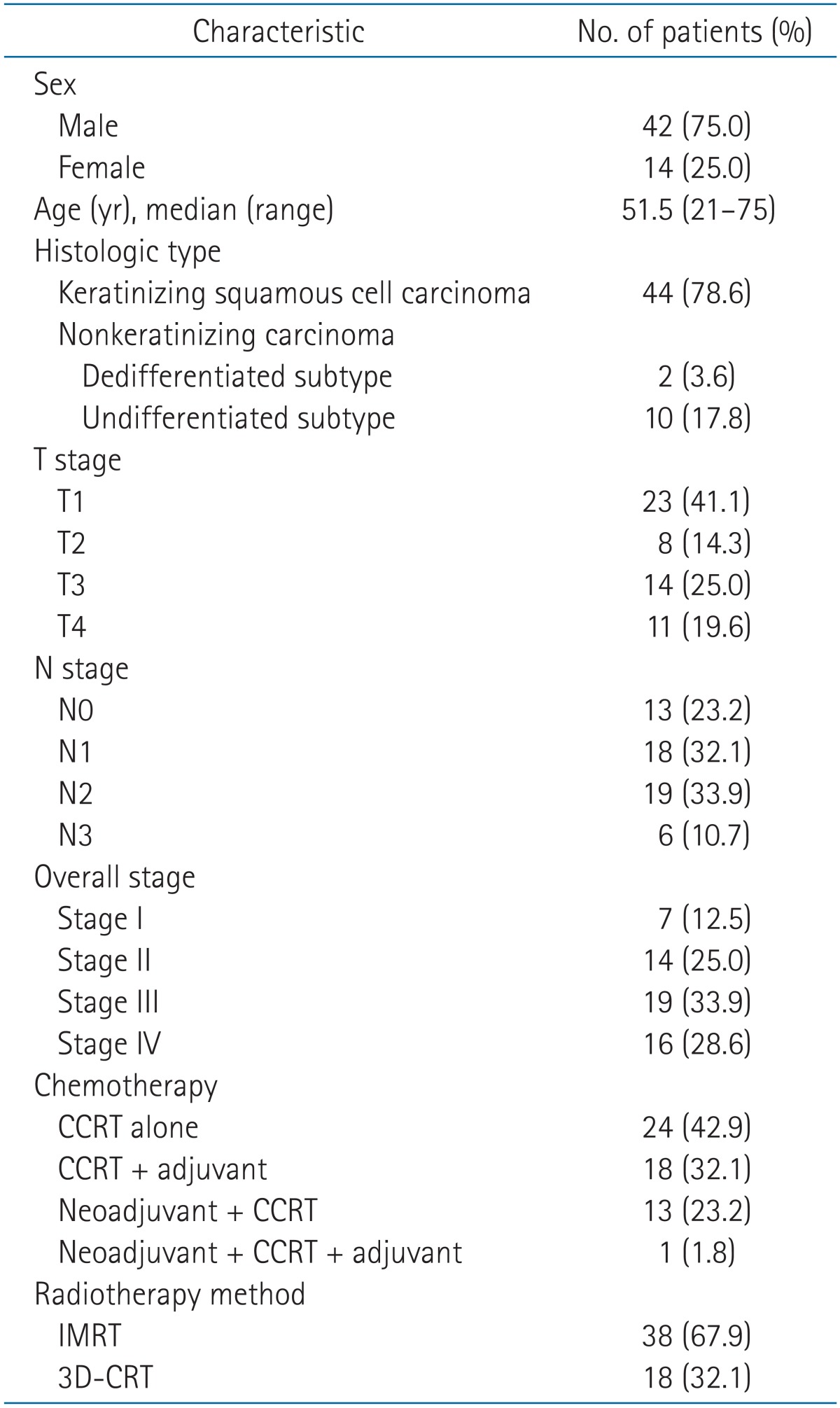
Forty-two male and 14 female patients were included in this analysis. Median age was 51.5 years old, with a range between 21 and 75 years. Pathologic findings included keratinizing squamous cell carcinoma in 44 patients, nonkeratinizing carcinoma (differentiated subtypes) in two patients and nonkeratinizing carcinoma (undifferentiated subtype) in 10 patients. Patient characteristics are listed in Table 1.
The distribution of T stages and N stages was as follows: 23 T1 patients; eight T2 patients; 14 T3 patients; 11 T4 patients; 13 N0 patients; 18 N1 patients; 19 N2 patients; and six N3 patients. There were seven (12.5%) patients with stage I; 14 (25.0%) patients with stage II; 19 (33.9%) patients with stage III; and 16 (28.6%) patients with stage IV (Table 1). Regarding the use of chemotherapy, 24 patients (42.9%) received CCRT alone, 13 patients (23.2%) received neoadjuvant chemotherapy with CCRT, and 18 patients (32.1%) received CCRT with adjuvant chemotherapy. The other one patient (1.8%) received neoadjuvant chemotherapy, CCRT, and adjuvant chemotherapy.
The median follow-up time was 38 months (range, 3 to 80 months). After completion of treatment, all patients achieved a complete remission.
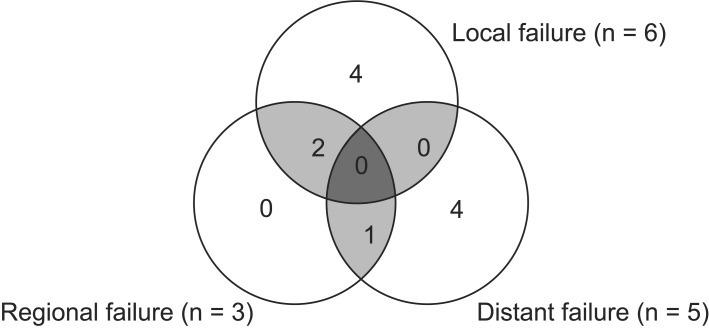
Overall disease failure at any site developed in 11 patients (19.6%). Among these patients there were six local failures (10.7%), three regional failures (5.4%), and five distant metastases (8.9%) (Fig. 2).
Six patients developed local recurrence: four patients failed in the nasopharynx, one patient experienced both local recurrence in the nasopharynx and in-field regional recurrence in the level II neck area, and one patient experienced a local failure described as marginal recurrence adjacent to the nasopharynx. At the time of this analysis, there was no out-of-field neck node failure in unirradiated neck levels. Table 2 summarizes the failure patterns of nodal recurrence.
Three patients had neck node failures. One patient (female/39 years old) had T1N2 disease with bilateral nodal disease at level II at the time of disease presentation. She was treated with CCRT (72.6 Gy of IMRT and 3 cycles XP). However, she complained of a left neck mass at 20 months after primary treatment, and fine-needle aspiration confirmed the presence of nodal recurrence. She was undergoing salvage neck node dissection and still survived without evidence of disease for 31 months. Another patient (male/59 years old) had T1N1 disease with multiple involvements of right neck level II-V nodal areas. He was treated with CCRT (72 Gy of 3D-CRT and 2 cycles XP). However, he had regional recurrence in contralateral neck nodes at 12 months after primary treatment and subsequently distant metastases were detected in the lung and the liver 15 months after primary treatment. He underwent salvage surgery and postoperative RT. Despite of the treatment, he died because of lung metastases occurring 22 months after primary treatment. Similarly, the third patient (male/68 years old) who had T2N0 disease with possible oropharynx extension had in-filed recurrence in the nasopharynx at 12 months after primary treatment (72 Gy of 3D-CRT and 2 cycles XP) and both neck failures in the electively irradiated area at 17 months after primary treatment. He received reirradiation on the recurrent neck region. However, several months later, multiple neck nodes, including intraparotid nodes, developed. Despite chemotherapy, he died due to disease progression 31 months after primary treatment.
Fig. 3 shows the clinical outcomes for all 56 patients. The 3-year LRC rate was 87.1%, and DFF rate was 90.4%; DFS and OS rates at 3 years were 80% and 86.8%, respectively. In subgroup analysis, there were no significant differences in 3-year actuarial rates of LRC, DFF, and OS according to sex, age, performance state, pathology, AJCC stage, fractionation size, overall radiation duration, and treatment method. No other potential prognostic factor was found to be predictive of outcome.
Discussion and Conclusion
There is an extensive submucosal lymphatic capillary plexus in the nasopharynx. Like most other head and neck primary cancers, lymphatic drainage of the nasopharynx is predominantly to the cervical lymph nodes. NPC has a higher incidence of cervical lymph node metastases compared with other head and neck cancers [2]. Because of the risk of lymph node metastasis, irradiation to the entire cervical lymph nodal drainage regions has been considered necessary. In a retrospective study reported by Lee et al. [9], 57 (30%) of 189 patients who did not receive elective neck irradiation subsequently developed cervical lymph node recurrence. However, none of the seven regionally treated patients relapsed. Considering the results from this study, radiation oncologists treated all neck lymph node levels comprehensively with definitive-intent radiation therapy or prophylactic irradiation. Even in the current era of IMRT, protocols by the Radiation Therapy Oncology Group (RTOG) still adopt comprehensive coverage of bilateral levels I to V lymph node regions in CTV, sparing level I only for N0 patients in the RTOG 0225 and 0615 trials [10
11]. However, irradiation of a large field to the neck is associated with severe complications. Early toxicities include radiation dermatitis and mucositis, especially if concurrent chemo-radiation is utilized. Late toxicities may include xerostomia, neck fibrosis, lymphedema, cranial neuropathy, and endocrine dysfunction [5]. If the reduced volume of neck irradiation can be safely implemented in patients with limited nodal disease burden, reduced volume of neck irradiation may improve the tolerability of RT, leads to greater patient compliance and quality of life. Advances in RT, including image guidance and IMRT, have also allowed oncologists to be highly selective and accurate in treatment delivery. In the IMRT era, it is often up to the clinical judgment of the radiation oncologist to decide how much of the neck irradiated volume and dose [4].
CT, MRI, and PET/CT imaging carry important roles in the diagnosis and staging of NPC and have improved the ability to detect nodal metastases and the knowledge about the patterns of lymphatic spread [12
13
14]. These imaging techniques help to assess the patterns of metastatic nodal spreads in the neck in NPC and to improve disease control due to better delineation of initial disease extent, better irradiation planning, and better treatment delivery.
Several investigators have reported that NPC cervical metastasis follows an orderly spreading pattern inferiorly along the neck, and skip metastases in the neck region are relatively rare [3
4
15
16]. King et al. [15] retrospectively reviewed the MRIs of 150 patients with newly diagnosed NPC and reported that direct lymphatic spread from the primary tumor to the neck nodes without involvement of retropharyngeal nodes was rare, occurring in only 6% of patients with neck node metastases in the upper neck. The study by Tang et al. [3], which was based on MRIs of 924 patients, showed that only two patients (0.3%) without retropharyngeal node or level II lymph node involvement had evidence of other lymph node involvement and lymph node metastases progress in an orderly fashion from higher level lymph nodes to lower level lymph nodes and rarely skip a site. They supposed that selective treatment of the neck lymph nodes for patients with NPC is feasible and prophylactic irradiation of level IV and supraclavicular fossa lymph nodes would not be necessary for patients who are negative for lymph node metastases. A meta-analysis of 2,920 patients from 13 studies using MRI as the main imaging modality by Ho et al. [4] showed that 85% of NPC patients had nodal involvement at the time of diagnosis. The most commonly involved nodal regions include retropharyngeal and level II lymph nodes. Nodal metastases followed an orderly pattern and the probability of skip metastasis between levels varied between 0.5% and 7.9%. According to these results, limiting coverage to the selective nodal regions and eliminating the irradiation to the entire neck could be considered.
As such, the necessity of large treatment fields for whole neck irradiation has been called into question. Review of different IMRT series showed marked variation in the coverage of level I and the lower neck. The individually tailored approach is increasingly advocated for select NPC patients. Gao et al. [17] conducted a retrospective study of 410 NPC patients staged as node negative by computed tomography. With a median follow-up of 54 months, they reported that only one patient (0.2%) experienced relapse outside the irradiation fields (level IV). Additionally, the reported 5-year OS rate, relapse-free survival rate, and DFS rate were 84.2%, 88.6%, 80.1%, respectively. They concluded that ENI by conventional technique to 50 to 56 Gy confined to RPN and levels II, III, and Va was safe for N0 NPC. The retrospective study by Zeng et al. [18] showed that the 5-year OS, nodal recurrence-free survival, and distant metastasis-free survival rates of the upper neck group and the whole neck group were 93.6% vs. 90.9% (p = 0.553), 99.4% vs. 99.0% (p = 0.278), and 98.8% vs. 94.9% (p = 0.128), respectively in 270 patients with N0 NPC who had undergone IMRT. A total of 3 neck recurrences were found, including 2 from the whole neck group and 1 from the upper neck group. The latter (0.6%) was an out-of-field recurrence. They also concluded that prophylactic irradiation to the upper neck (levels II, III, and VA) may be feasible for patients with neck lymph node-negative NPC. Li et al. [19] reported the clinical outcomes of 301 patients with node-negative NPC. This randomized clinical trial showed that the 3-year OS, relapse-free survival, and metastasis-free survival rates were not different between upper vs. whole-neck prophylactic irradiation in node-negative NPC patients. They insisted that prophylactic upper neck irradiation is sufficient for patients with node-negative NPC. Chen et al. [20] reported the results of a prospective phase 2 study examining the effects of a tailored ENI approach in patients with N0-1 NPC. This study included not only node-negative patients but also patients with N1 disease as staged by CT who were treated with IMRT but did not receive ENI to level IV and Vb nodes. Seven out of 212 patients (4 in-field and 3 out-of-field) developed nodal failure. The 5-year regional control rates of the entire group, N0 patients, and N1 patients, were 95.6%, 98.2%, and 91.3%, respectively. They concluded that the rate of out-of-field nodal failure when omitting ENI to levels IV and Vb in the clinically negative necks of patients with N0-1 NPC was extremely low.
In addition to N0 and N1 patients, our study also included patients with N2 and N3 (involvement of upper neck nodal area) staged by PET/CT. The ENI included retropharyngeal and level II lymph nodes in all patients, and only encompassed the echelon inferior to the involved level to eliminate the entire neck irradiation. No nodal failures in the omitted ENI sites were observed in this study. Three patients (5%) developed nodal failure: two nodal failures (3.6%) were in-field recurrence occurred in ENI site, and one patient (1.8%) developed lymph node recurrence in level II that was inside of the radiation field delivering dose of 72.6 Gy. In our study, the causes of failure were, in order of frequency, local recurrence, distant metastasis, and regional recurrence (Fig. 2). Regional recurrence alone was none. Therefore, the individually tailored ENI was shown to be safe and feasible.
Omission of certain neck nodal areas (e.g., levels I, IV, and Vb) can reduce the RT dose to surrounding normal tissues, especially the thyroid gland in the low neck. It is always advisable to spare as much normal surrounding tissue as possible. The main advantage is the possibility of reducing xerostomia by omitting level I. Despite evidence of almost full recovery of parotid salivary flow after IMRT, a study by Pow et al. [21] showed that oral health-related quality of life of NPC patients after IMRT was still significantly worse than at baseline because whole salivary flow had only recovered by 40%; thus, dose reduction or sparing the submandibular and/or sublingual glands from radiation damage during NPC treatment is needed. Although our study lacked an analysis of complications and toxicity, we believe that the rates of certain late toxicities, including skin dystrophy, subcutaneous neck fibrosis, carotid occlusive disease, and xerostomia, would be low.
The NCCN guideline of head and neck cancers [22] recommends that elective irradiation to low risk and intermediate risk sites requires 44 Gy (2.0 Gy/fraction) to 63 Gy (1.6ŌĆō1.8 Gy/fraction), depending on the estimated level of tumor burden. NPC have the better radiosensitivity when compared with the other squamous cell carcinomas of the head and neck [23]. And the combination of concurrent chemotherapy also enhance the radiation response [24
25]. In 3D-CRT of our study, the dose of median 39.6 Gy (range, 39.6 to 45 Gy; 1.8 Gy/fraction) was used for ENI of the low risk neck because of the spinal cord tolerance dose. Our study reported that two patients who were received a dose of 39.6 Gy experienced in-field recurrence occurred in PTV2 ENI site. In the era of IMRT, we used a higher dose of 49.5 Gy (EQD2 44.2 Gy10) for ENI of low risk neck in order to improve the regional control rate.
The primary limitation of our study is the small sample size, which was restricted to include patients who received the individually tailored field of ENI instead of whole neck irradiation in a single institution. Because of the retrospective nature of the review, the results were subject to data collection and interpretation bias. Another limitation of this study was that the chemotherapy was not administered in a controlled manner but was instead used at the discretion of the attending physician. Clinical studies have confirmed that chemotherapy may eradicate subclinical disease and improve LRC, especially for locoregional advanced disease [24
25]. Future studies should address this issue.
In conclusion, no patient developed nodal failures in the omitted ENI site. Results from our study were comparable to those with whole neck irradiation reported by other centers. Our investigation demonstrates the reduced volume approach for ENI appears to be a safe treatment approach in NPC. We expect that minimizing the irradiated neck volume could potentially reduce the risk of toxicity and improve patient quality of life.