Introduction
Lung cancer is one of the most common causes of cancer-related death not only in Korea but worldwide, and non-small cell lung cancer (NSCLC) accounts for approximately 85% of all lung cancer cases [1-4]. Several modalities are currently used to treat NSCLC. Surgical resection is the treatment of choice for early-stage NSCLC, while adjuvant chemotherapy or chemoradiotherapy (CRT) is recommended for selected patients [5-7]. For locally advanced NSCLC, multimodality treatments including definitive CRT and surgical resection with neoadjuvant CRT are usually adopted [8-11]. After undergoing these curative approaches, 3%–20% of patients have been reported to develop locoregional recurrence (LRR) without distant metastases [5-11]. Salvage radiotherapy (RT) with or without concurrent chemotherapy has been used to treat patients with postsurgical LRR of NSCLC [12-14]. However, some patients receive RT during the initial treatment course, and re-irradiation in this patient group may be challenging as overlapping re-irradiation volumes could potentially cause severe radiation injury [15].
Technological advances in radiotherapy, including three-dimensional conformal radiotherapy and intensity-modulated radiation therapy (IMRT), have enabled the delivery of high-dose re-irradiation, and several studies have reported the efficacy and toxicity after re-irradiation for LRR of NSCLC. In these studies, the 2-year overall survival (OS) rate ranged from 32.6% to 39.4%, while the incidence of pulmonary toxicity of ≥grade 3 ranged from 0% to 10% [16-18]. Furthermore, proton beam therapy (PBT) can offer clinical advantages compared with conventional photon therapy. It has a unique depth-dose curve with a dose peak (Bragg peak) at a well-defined depth in tissue. This feature enables substantial reductions in doses delivered to the normal tissues proximal and distal to the target volume, which makes it possible to spare normal tissues that overlap in previously irradiated fields and to deliver escalated doses to tumors during salvage treatment [18-21]. Several studies examined the efficacy of re-irradiation with PBT for NSCLC, and the 2-year OS rate was reported to be 32.6%–43.0%. However, the majority of these studies have been conducted in the United States [18,22-25]. In this study, we aimed to retrospectively analyze our institutional experience of salvage PBT for locoregionally recurrent NSCLC in terms of survival outcomes and toxicity.
Materials and Methods
1. Patients
We retrospectively reviewed the medical records of patients with locoregionally recurrent NSCLC treated with salvage PBT between January 2016 and December 2019. A retrospective study of patients with PBT was approved by the Institutional Review Board of Samsung Medical Center (No. 2020-01-034). Patients with initial stages I–III NSCLC who underwent curative intent therapy, with clinically or pathologically confirmed LRR, with no evidence of distant metastasis, and who received PBT for locoregionally recurrent NSCLC with curative intent were considered eligible for the study. LRR was defined as recurrence of tumor in ipsilateral lung or regional lymph nodal area [22,26]. We identified 53 patients who satisfied the inclusion criteria. When recurrence was suspected, the patient underwent chest computed tomography (CT) with or without 18-fluorodeoxyglucose positron emission tomography-CT. Pathologic confirmation of recurrence was performed in 24 (45.3%) patients. All patients were re-staged according to the 8th edition of the American Joint Committee on Cancer staging system. If the patient had a previous history of RT, the failure patterns in the previous RT field were classified into in-field failure, marginal failure, and out-field failure. In-field failure was defined as recurrences in which the geometric center of the mass was within the 50% isodose line. Meanwhile, marginal failure was defined as recurrences in which the geometric center of the mass was between the 25% and 50% isodose line [18,22]. After salvage PBT, patterns of failures were classified into local, marginal, and distant failure. Local failure was defined as a failure within the irradiated volume. Regional failure was defined as recurrence within ipsilateral lung lesion or the regional lymph nodes of the intrapulmonary, peribronchial, hilum, mediastinum or supraclavicular region outside of the original planning target volume (PTV). Failures occurring outside of these defined local and regional failures were considered distant failures [25,27,28].
2. Treatment
All patients underwent CT simulation in the supine position at a thickness of 2.5 mm. The gross tumor volume (GTV) included all recurrent lesions, while the internal target volume (ITV) was delineated based on all respiratory phases using a four-dimensional CT. The clinical target volume (CTV) was delineated by adding a 5- to 7-mm margin from the ITV, and the margins were modified in accordance with the adjacent organs if necessary. The PTV was delineated by adding a 5-mm margin to the CTV to account for setup uncertainties. The median GTV and CTV were 14.9 cm3 (range, 2.3 to 759.5 cm3) and 71.2 cm3 (range, 13.3 to 1,200.7 cm3), respectively. The median total dose was 64.0 cobalt gray equivalent (CGE) (range, 45.0 to 70.0). The median biologically equivalent dose (BED10) was 80.5 Gy10 (range, 58.5 to 115.2 Gy10). RayStation (RaySearch Laboratories, Stockholm, Sweden) was the system used for treatment planning. PBT was delivered using the proton therapy system at Samsung Medical Center (Sumitomo Heavy Industries, Tokyo, Japan). Most of the patients (n = 47; 88.7%) received pencil beam scanning PBT, while the remaining 6 patients (11.3%) received passive scattering PBT. All treatment sessions were delivered under daily image guidance with orthogonal kilo-voltage X-ray imaging or cone-beam CT using VeriSuite (MedCom, Darmstadt, Germany). Concurrent chemotherapy was administered in 17 (32.1%) patients.
3. Endpoints and statistical analyses
Patients underwent regular follow-up examinations, including physical examination, hematologic studies, and chest CT. Tumor response to radiotherapy was evaluated using the revised Response Evaluation Criteria in Solid Tumors guidelines (version 1.1). The endpoints included OS, progression-free survival (PFS), and local control (LC). All endpoints were calculated from the start date of salvage PBT to the date of the last follow-up, death, or progression. The failure patterns following salvage PBT were classified into local failure, regional failure, and distant failure. Treatment-related toxicity was graded according to the National Cancer Institute (NCI) Common Terminology Criteria for Adverse Events version 5.0.
Survival outcomes were calculated using the Kaplan-Meier method and compared using the log-rank test for univariate analysis. The Cox proportional hazard regression model was used for multivariate analysis. Multivariate analysis was performed on variables that showed a probability value of <0.1 or on those that were thought to be relevant. Fisher exact test was used to compare the patterns of failures or toxicities after salvage PBT according to the site of disease recurrence in the previous RT field. Statistical analyses were performed using SPSS Statistics version 25.0 (IBM Corp, Armonk, NY, USA). A p-value of less than 0.05 was considered significant.
Results
Patients’ baseline characteristics are summarized in Table 1. The median age was 67 years (range, 44 to 86 years), and 47 (88.7%) of the total patients were men. Thirty patients (56.5%) had a smoking history of more than 30 pack-years. With regard to the histologic types, 26 patients (49.0%) had squamous cell carcinoma, 25 (47.2%) had adenocarcinoma, and 2 (3.7%) had large-cell carcinoma. In terms of initial staging, 22 patients (41.5%) had stage I, 8 (15.1%) had stage II, and 23 (43.4%) had stage III. The initial treatments were surgery in 31 (58.5%), definitive CRT in 12 (22.6%), and definitive RT in 10 (18.9%) patients. Among the 31 patients who underwent surgery, 3 (5.7%) received neoadjuvant CRT, while another 3 (5.7%) had adjuvant CRT.
The median disease-free interval (DFI), defined as the period from the start of previous treatment to the period when recurrence was diagnosed, was 14 months (range, 3 to 112 months). With regard to the staging of cancer recurrence, 11 patients (20.8%) had stage I, 11 (20.8%) had stage II, and 31 (58.4%) had stage III. Overall, 41 patients (77.3%) had 1 episode, 11 (20.8%) had 2 episodes, and 1 (1.9%) had 3 episodes of cancer recurrence. Thirty-seven patients (69.8%) had a previous history of RT. Among them, 18 patients (48.7%) had in-field recurrence, 12 (32.4%) had marginal field recurrence, and 7 (18.9%) had out-field recurrence.
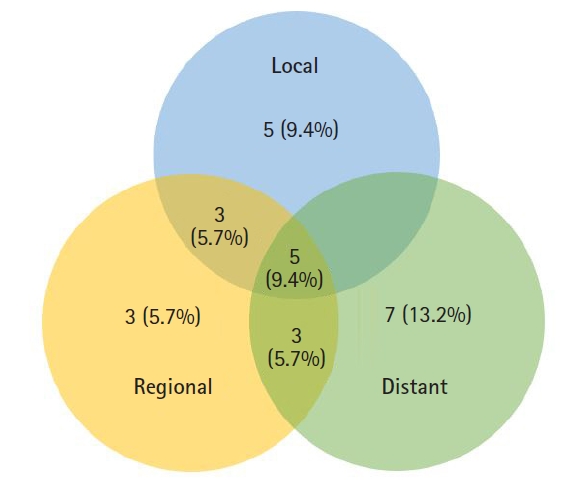
The median follow-up time after salvage PBT was 15.0 months (range, 3.5 to 49.3 months). During the follow-up period, 26 patients (49.1%) experienced disease progression. Fig. 1 shows the patterns of failures following salvage PBT. Local failure with or without regional/distant failure was observed in 13 (24.5%) patients. Among the 18 patients who had disease recurrence in the previous RT field (in-field failure), 6 (33.4%) experienced local failure; meanwhile, 7 (20.0%) among the other 35 patients had local failure (p = 0.326, Fisher exact test). In contrast, out-field recurrence was less frequent in patients with disease recurrence in the previous RT-field (in-field failure) than in those with other types of recurrence: 5 (27.8%) vs. 15 (42.9%) (p=0.283, Fisher exact test).
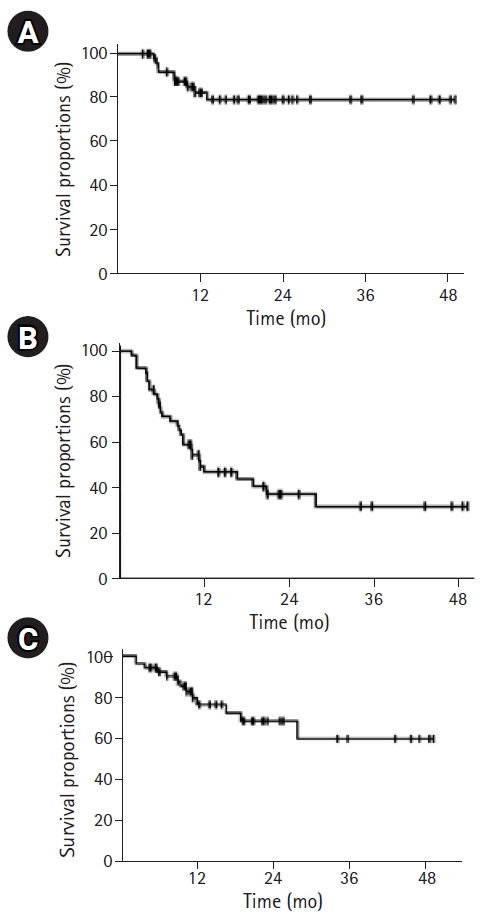
The 2-year OS, PFS, and LC rates were 79.2%, 37.1%, and 68.2%, respectively (Fig. 2). Univariate analysis revealed that shorter DFI (≤12 months vs. >12 months; p = 0.015) and larger CTV (>80 mL vs. ≤80 mL; p = 0.014) were associated with poor OS (Table 2). In patients with disease recurrence in the previous RT field (in-field failure), the 2-year LC rate was 54.8%, which was lower than that of patients with other types of recurrence (74.1%), although the difference was not significant (p = 0.238). In the multivariate analysis, shorter DFI (hazard ratio = 5.876; 95% confidence interval, 1.002–34.448; p = 0.040) and larger CTV (hazard ratio = 7.126; 95% confidence interval, 1.236–41.070; p = 0.028) were independent prognostic factors for OS (Table 3).
Most patients tolerated salvage PBT, except 1 patient (1.9%) who could not complete the planned PBT due to grade 3 radiation esophagitis. None of the patients had grade 4 or 5 toxicity. Pulmonary toxicity was the most common treatment-related toxicity: 9 patients (17.0%) had grade 1, 18 (34.0%) had grade 2, and 4 (7.5%) had grade 3. Grade 3 esophagitis and dermatitis occurred in 2 (3.7%) and 3 (5.7%) patients, respectively (Table 4). Among the 8 patients who experienced grade 3 toxicity, 4 had disease recurrence in the previous RT field (in-field failure), 3 had pulmonary toxicity, and 1 had esophagitis. The remaining 4 patients experienced dermatitis (n = 3), esophagitis (n = 1), and bronchial obstruction (n = 1); 1 patient experienced both grade 3 esophagitis and dermatitis.
Discussion and Conclusion
In this retrospective study, we analyzed the treatment outcomes of salvage PBT with or without chemotherapy for LRR of NSCLC. Several previous studies analyzed the survival outcomes and toxicities after salvage RT in patients with LRR of NSCLC, and the OS in these studies ranged from 32.6% to 73% [12-14,16-18,22-25].
Some studies have demonstrated favorable outcomes after salvage RT in patients with postsurgical LRR of NSCLC [12-14]. In these studies, the 2-year OS rate ranged from 56% to 73%. The current study not only included patients with postsurgical recurrence but also those with post-RT recurrence, with a 2-year OS of 79.2%. Overall, 31 patients underwent surgical resection at initial treatment, and 6 received adjuvant or neoadjuvant CCRT. The 2-year OS rate of the 31 patients was 87.7%, which was higher than that of patients who had undergone definitive CCRT or RT alone at initial treatment (60.6% and 77.8%; p = 0.065).
Meanwhile, in patients with a previous history of RT, high-dose re-irradiation could result in severe treatment-related toxicity or low survival outcomes. As radiotherapeutic techniques have been developed, high-dose re-irradiation is feasible using highly conformal RT [16-18] (Table 5). Hong et al. [16] analyzed the treatment outcomes of 31 patients who received high-dose conformal re-irradiation. The 2-year OS and LC were 39.4% and 43.7%, respectively. In terms of treatment-related toxicity, none of the patients experience ≥grade 3 acute toxicity, while one patient developed grade 3 late pericarditis. Another retrospective study analyzed 102 patients who underwent re-irradiation using IMRT or PBT as treatment for intrathoracic recurrence of NSCLC [18]. In this study, the 2-year OS and local failure-free survival rates were 32.6% and 34.2%, respectively. Grade 3 esophageal and pulmonary toxicities developed in 7 (7%) and 10 (10%) patients, respectively. The study demonstrated that a higher composite dose was associated with greater toxicity in patients who underwent PBT re-irradiation for intrathoracic recurrence of NSCLC [22].
PBT is expected to reduce the overlapped volume in case of re-irradiation, and several studies have reported the treatment outcomes after PBT irradiation. A multi-institutional prospective study enrolled 57 patients who had NSCLC recurrence in or near the previous radiation field from three proton centers [23]. Although the 2-year OS and PFS were 43% and 38%, respectively, this study showed a relatively higher incidence of ≥grade 3 toxicity (n = 24; 42%). The researchers showed that central overlapped volume, mean heart dose, mean esophagus dose, and concurrent chemotherapy were significantly associated with higher rates of ≥grade 3 toxicity. However, another prospective registry study reported that 6% of the total patients who had partial overlap in the previous radiation, and PBT re-irradiation fields showed acute grade 3 toxicity [24]. The study did not indicate the 2-year survival outcomes, while the 18-month OS and local relapse-free survival rates were 34.1% and 30.9%, respectively.
Based on these results, the treatment outcomes after re-irradiation appeared to be somewhat less favorable than those after salvage RT for patients with postsurgical recurrence without previous RT history. But, the current study which included patients with or without previous RT history, has shown no significant difference in the treatment outcomes between these patient groups according to previous RT history (Table 2). Patients with recurrent lesions in the previous RT field (in-field failure) tended to have slightly worse survival outcomes, which was not statistically significant. Nonetheless, the 2-year OS rate of 37 patients with previous RT history was 72.9%, which was higher than that reported in previous re-irradiation studies (33%–43%) [16,18,23,24] (Table 5). Meanwhile, previous re-irradiation studies showed an LC rate of 31%–44% at 1.5–2 years [16,18,24], while the current study reported an LC rate of 65.6% at 2 years (Table 5). Furthermore, patients with recurrent lesions in the previous RT field (in-field failure) had a tendency to experience recurrence in the RT field of salvage PBT, although it was not significant (p = 0.326, Fisher exact test).
Considering the technical aspects, 88.7% of the patients in the present study received pencil beam scanning proton therapy. IMPT, which is based on the scanning beam technique, is expected to further improve the rate of normal organ sparing [19]. The treatment outcomes following IMPT re-irradiation were recently published [25]. Only 2 patients (7%) experienced late grade 3 pulmonary toxicity, and the 18-month OS and freedom from local failure rates were 54% and 78%, respectively, which were comparable with those reported in the present study. In the present study, grade 3 toxicities were observed in 8 patients (15.1%): pulmonary (n = 4; 7.5%), esophagitis (n = 2; 3.7%), and dermatitis (n = 3; 5.7%), respectively (Table 4). In the 18 patients with in-field recurrence, grade 3 toxicity was observed in 4 patients (22.2%); meanwhile, only 11.4% (n = 4) of the other 35 patients experienced grade 3 toxicity (p = 0.299, Fisher exact test). Therefore, the occurrence of severe toxicity must be avoided when re-irradiating the overlapped volume, and an effort must be made to further reduce the risk of toxicity.
In terms of prognosis, several factors such as DFI, recurrent tumor volume, concurrent chemotherapy, and re-irradiation dose including BED have been reported to be associated with survival outcomes [12-14,18,25]. In the present study, CTV of >80 mL and DFI of ≤12 months were independently associated with worse OS.
However, this study has some limitations. First, this was a retrospective study. An intrinsic bias possibly exists in this study. For example, the toxicity rate might be underestimated. Second, the number of patients included was small, and the follow-up period was not long. These factors weakened the statistical power. Therefore, a prospective study with a large sample size is needed. Third, significant heterogeneity was observed in the patient population in terms of initial therapy, salvage therapy, RT technique, and others. Finally, we only included patients treated with PBT; hence, we cannot directly compare the outcomes with those of patients who underwent other modalities such as IMRT, and then we cannot conclude that PBT is superior to IMRT in terms of toxicity profile (Table 5). In this regard, another retrospective study comparing PBT and IMRT as salvage re-irradiation might be helpful, but potential selection bias could still exist.
In conclusion, although some potential limitations were noted, salvage PBT as treatment for LRR of NSCLC showed favorable survival outcomes and treatment-related toxicities. Larger CTV and shorter DFI were independent unfavorable prognostic factors for OS. Even, patients with previous RT history and in-field recurrence also showed comparable survival outcomes and the incidence of ≥grade 3 toxicities, though it was slightly worse. Careful selection of patients considering the risks and benefits should be accompanied to apply PBT for patients with LRR of NSCLC, especially in re-irradiation case.