Patterns of failure and clinical outcomes of post-operative buccal mucosa cancers treated with adjuvant ipsilateral radiotherapy
Article information

Abstract
Purpose
Adjuvant radiotherapy (RT) in buccal mucosa cancers is guided by histopathological factors. The decision to treat ipsilateral or bilateral draining lymph node is on physician discretion and guidelines do not have a defined indication regarding this. We aimed to analyze the failure patterns and survival in buccal mucosa cancers treated with adjuvant ipsilateral RT.
Materials and Methods
One hundred sixteen cases of post-operative buccal mucosa cancers—pT3 or more, node positive, close margins (1–5 mm), lymphovascular invasion positive, perineural invasion positive, depth of invasion >4 mm—treated with RT to primary and ipsilateral nodes from May 2013 to May 2019 were retrospectively analyzed. Patients were treated to a dose of 60–66 Gy (44 Gy in the first phase and a coned down boost of 16–22 Gy in the second phase) with three-dimensional conformal radiotherapy on a linear accelerator. Primary end point was to assess control rates and secondary end point was to evaluate the overall survival (OS) and disease-free survival (DFS) outcomes.
Results
Median age was 46 years with male; female ratio of 110:6. The edition of the American Joint Committee on Cancer stage distributions were I (3.4%), II (34.4%), III (24.1%), and IV (37.9%). At a median follow-up of 22 months, crude rates of local failure, regional failure, and contralateral neck failure were 9.4%, 10.3%, and 3.4%, respectively. The 2-year contralateral neck control rate was 94.9%. Pathological positive node portended poorer OS (86.6% vs. 68.6%; p = 0.015) and DFS (86.5% vs. 74.9%; p = 0.01).
Conclusion
Incidence of contralateral recurrence with ipsilateral irradiation in buccal mucosa cancers is low with descent survival outcomes, particularly in node negative cases.
Introduction
Oral cavity cancers account for approximately 0.35 million new cases and 0.18 million deaths annually, worldwide [1]. India accounts for roughly one-third of the new cases and around half the number of deaths [1]. Buccal mucosa cancers accounts for around half of these cancers [2,3]. Standard therapy for buccal mucosa cancers is optimal surgical resection followed by adjuvant treatment [4]. Adjuvant radiotherapy after surgery is indicated in cases with pathological tumor size of pT3 or more, pathological node positivity, close margins, lymphovascular invasion (LVI) positive, perineural invasion (PNI) positive, depth of invasion (DOI) >6 mm [5]. Around 60% cases of buccal cancers present with advanced stage and patients tend to have multiple risk factors [6,7]. Post-operative radiotherapy with or without chemotherapy is the standard of care after resection of locally advanced carcinomas, as these patients are higher risk for locoregional relapse [8]. The volumes for adjuvant radiotherapy generally include the primary tumor bed, ipsilateral and or contralateral nodal volumes. Standard guidelines regarding the inclusion or exclusion of contralateral draining lymph nodes as elective volume in adjuvant radiotherapy does not exist and are mostly guided by clinician discretion. For patients with clear margins and no extracapsular extension, elective contralateral neck radiation is suggested for cases with high risk like advanced disease approaching midline and multiple positive nodes in the ipsilateral neck which increase the risk of nodal recurrence in the contralateral neck [9]. However, contralateral neck irradiation is not routinely performed [9-11]. Various clinical studies opine that ipsilateral neck dissection results in good outcomes with very limited contralateral neck failure in buccal mucosa cancers [12,13] setting the pretext for ipsilateral adjuvant radiotherapy in selected subset of buccal mucosa cancers.
There are no detailed guidelines regarding the management of buccal cancers in terms of ipsilateral or bilateral neck irradiation. However, selected subset of buccal mucosa cancers presenting with limited number of risk factors and favourable prognosis can be treated with ipsilateral radiotherapy to neck nodes and tumor bed, thereby limiting toxicity but without impairing outcomes. Literature on patterns of failure in these group of patients is sparse. The general practice followed at our institute is to irradiate the ipsilateral face and neck in patients intermediate risk disease [14]. We therefore conducted a retrospective analysis of prognostic factors, failure patterns and survival outcomes in these cohort of buccal cancers treated with ipsilateral irradiation at our institute and tried to identify subgroup(s) with poor prognosis suitable for more aggressive therapeutic approach.
Methods and Materials
1. Patients
It was a retrospective analysis of buccal mucosa squamous cell carcinoma patients, treated with surgery and radiotherapy to primary and ipsilateral nodes from May 2013 to May 2019. The data of 1,400 patients of head and neck cancer treated with radiotherapy was retrieved from the departmental archives of radiation oncology department. From this data, 116 cases of buccal mucosa cancers who underwent curative resection and received irradiation to primary tumor and ipsilateral neck were identified. The consort diagram representing the actual number of patient data retrieved has been mentioned in Fig. 1. All the records were reviewed for each patient: age, gender, site of primary tumor, stage as per the 7th edition of the American Joint Committee on Cancer [15], histological findings after surgery, local and regional recurrence in ipsilateral and contralateral neck, disease-free survival (DFS) and overall survival (OS). The patients receiving neoadjuvant chemotherapy were excluded. The patients having tumor in any site other than buccal mucosa and multiple oral cavity and/or head and neck cancers or previously treated oral cancers were also excluded from the study.

Consort diagram depicting the selection of patients for the present analysis.
2. Treatment
All patients underwent adequate resection of the primary tumor and neck nodes. Surgery of the primary tumor consisted of wide local excision or composite resection with/without marginal or segmental mandibulectomy depending upon the extent of the disease. Neck dissection included either supra-omohyoid or modified radical neck dissection. Patients with any or more of the following risk factors were included in the study: pathological tumor size of pT3 or more, pathological node positivity, close margins, LVI positive, PNI positive, DOI >6 mm. While evaluating various outcomes in terms of DOI, <12 mm and >12 mm were use as parameters [13]. All patients had lateralized primary tumors with adequate surgical resection.
Clinical target volumes (CTV) consisted of the post-operative tumor bed with a margin of 1 cm and the ipsilateral nodal volumes. The levels of the nodal volumes were decided as per the risk factors present in the post-operative histopathological factors and the possible sites of clinical and nodal spread. The planning target volume (PTV) included CTV with a 0.5-cm uniform margin to account for set up and motion errors. Radiotherapy was delivered using 6-MV photons to a dose of 60–66 Gy, using a 2-Gy dose fractionation, one fraction per day, 5 days per week by using linear accelerator (Infinity and Synergy; Elekta, Crawley, UK) with a collimator leaf width of 1 cm at the isocentre. Patients were treated with three-dimensional conformal radiotherapy using either parallel opposed anterior-posterior oblique fields in a single phase to a dose of 60–66 Gy respecting the spinal cord tolerance or using anterior and lateral field in two phases, in which 44 Gy was delivered in the first phase and a coned down boost of 16–22 Gy was delivered in the second phase. The median dose of radiotherapy was 60 Gy (range, 58 to 66 Gy). All patients were followed up on a regular basis: monthly once for first 6 months, every 2 months for the next year, every 3 months for the third and fourth years, and then 6 months to annually, thereafter.
3. Statistics
Primary end point was to assess local and regional control rates and secondary end point was to evaluate the survival outcomes: OS, DFS, and distant metastasis-free survival (DMFS). Locoregional failure was defined as the appearance of tumor in the post-operative bed or cervical node metastasis or both. All time intervals were calculated from the date of registration in the radiation oncology or surgical oncology department (whichever was earlier) to the date of event of interest. OS was measured from the date of registration to the date of death from any cause. DFS was defined as the time from the day of registration to date of failure (either locoregional or distant or both) or death. DMFS was defined as the time interval until the development of distant metastasis. Statistical analysis was performed with SPSS statistical software package for Mac (version 23.0; IBM, Armonk, NY, USA). All survival analyses were performed using Kaplan-Meier method. Log-rank test was used to test the statistical significance of differences in the survival and control rates. p < 0.05 was considered statistically significant. All potential prognostic factors were analyzed. Cox regression analysis was used to perform multivariate analysis on factors found significantly associated with outcomes in univariate analysis.
Results
1. Clinicopathological factors
Median age was 46 years (range, 28 to 80 years) with male; female ratio of 110:6. All patients underwent ipsilateral neck dissection, except three patients who underwent bilateral neck dissection. Stage of the patients in terms of pathological tumor size, pathological nodal size and overall pathological staging have been mentioned in Table 1. Four patients of stage I (pT1N0) were taken up for adjuvant radiotherapy as they had one or more high-risk factors for recurrence (two of them had PNI, one had lymphovascular space invasion and three patients had DOI more than 10 mm). Fifty-six patients (48.27%) had clinically positive nodes, but 48/116 (41.3%) were pathologically positive. The ipsilateral neck was irradiated in 113 cases (97.4%), whereas 3 cases received radiotherapy only to the primary tumor bed.
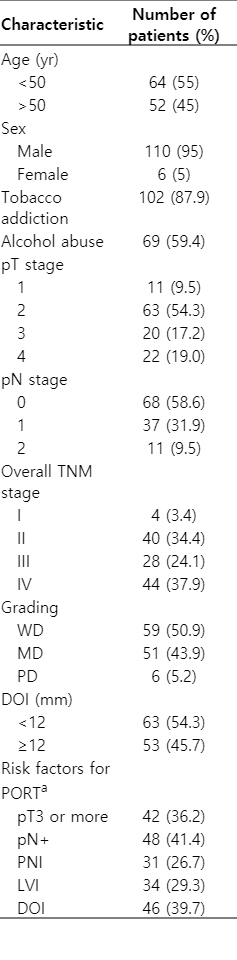
Clinicopathological factors (n = 116)
2. Locoregional control, local control, and regional control
Median follow-up was 22 months (range, 6 to 163 months). The 2-year locoregional control (LRC), local control (LC), and regional control (RC) rates were 80.9%, 88.4%, and 89.5%, respectively. There were 23 locoregional failures. The crude LC and RC rate were 90.5% and 89.7%, respectively. There was no significant difference in LRC, LC, and RC with clinicopathologic factors like age, sex, pT stage, overall tumor stage, LVI, PNI, DOI or grade (Table 2). There was statistically significant difference in 2-year LRC rates for different nodal stages (pN0 vs. pN1 vs. pN2: 86.1% vs. 71.5% vs. 77.9%; p = 0.036) (Fig. 2). The factor significantly influencing LRC rate (pN0 vs. pN1+2: 86.1% vs. 72.9%; p = 0.016) and RC rate (pN0 vs. pN1+2: 100% vs. 81.8%; p = 0.037) was pathological nodal staging, although it did not influence the LC rates.
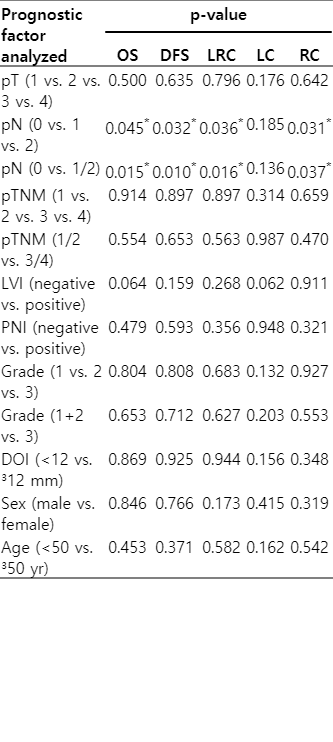
Variation of outcomes with prognostic factors in univariate analysis
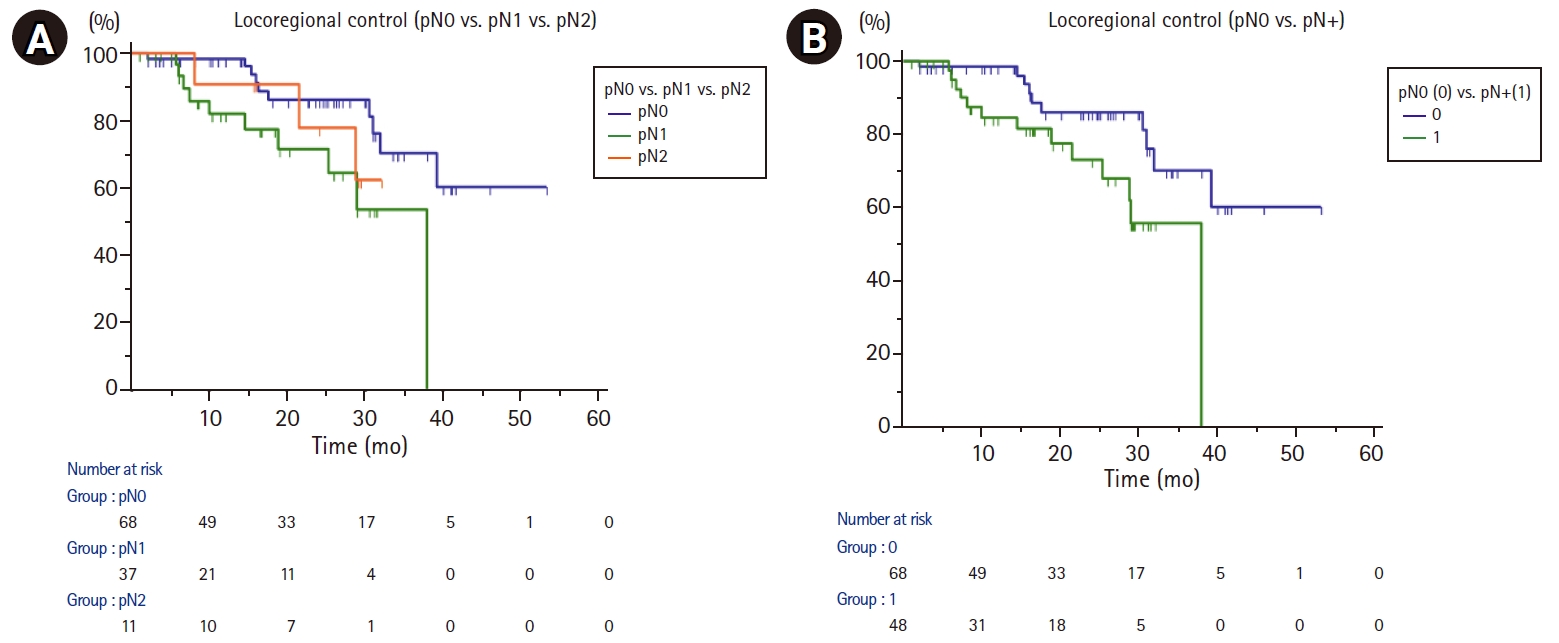
Kaplan-Meier curves depicting the variation of locoregional control with (A) pN (0 vs. 1 vs. 2) and (B) pN (0 vs. 1/2).
3. Overall survival
The 2-year OS for the entire cohort was 79.5%. The number of events in T1, T2, T3, and T4 were 4/11, 14/63, 3/20, and 4/22, respectively, for calculation of OS. On performing an univariate analysis, tumor stage, pathological tumor size, LVI, PNI and DOI didn’t impact the OS (Table 2). However, statistically significant results were noticed with pathological nodal staging. There was statistically significant improved outcomes with pathological node negativity. Presence of pathologically positive nodes was significantly inversely correlated with OS; (pN0 vs. pN1+2: 86.6% vs. 68.6%; p = 0.015; Fig. 3A) and (pN0 vs. pN1 vs. pN2: 86.6% vs. 71.7% vs. 64.9%; p=0.045), respectively.
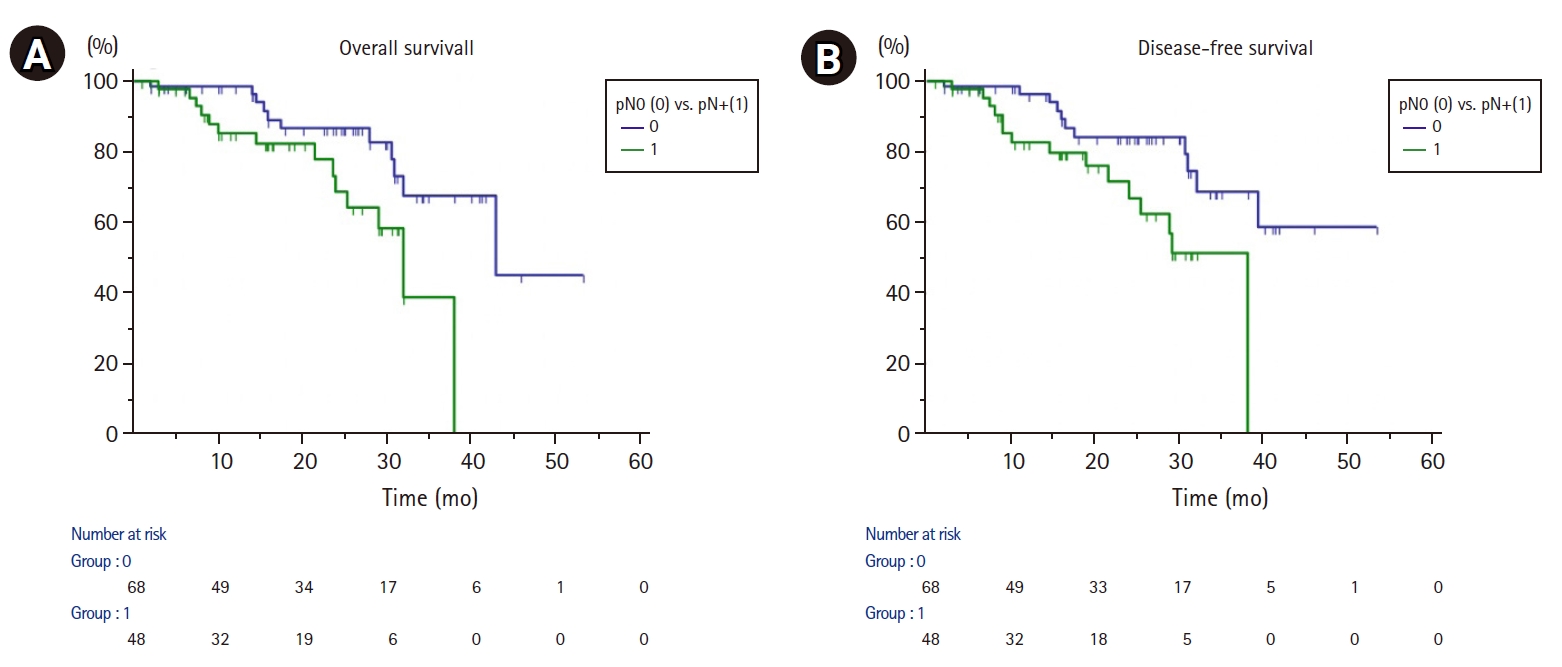
Kaplan-Meier curves depicting (A) overall survival and (B) disease-free survival variation with nodal status.
4. Disease-free survival
The 2-year DFS rate was 77.4%. The percentage of events in pN0, pN1, and pN2 cases for calculation of DFS were 11/68 (16%), 11/37 (30%), and 4/11(36%), respectively. Among the prognostic factors, only pathological N staging was associated statistically significant decrease in 2-year DFS rates with nodal positivity; (pN0 vs. pN+: 86.5% vs. 74.9%; p = 0.010; Fig. 3B) and (pN0 vs. pN1 vs. pN2: 84.3% vs. 69.6% vs. 64.9%; p = 0.032), respectively.
5. Failure patterns
Twenty-three patients had locoregional failures. Of these 30.4% (7/23) cases failed within 12 months, while 60.8% (14/23) patients failed within 2 years. Eleven cases had isolated local failure without regional failure, while 12 had isolated regional failure. Four patients had contralateral neck failures. Five patients had isolated distant failures. The crude contralateral lymph node failure (CLNF) rate and 2-year contralateral neck recurrence control rate were 3.4% (4/116) and 94.9%, respectively. The most significant factor affecting CLNF was nodal status. Statistically significant difference in CLNF rates were found with higher nodal burden (pN0 vs. pN1 vs. pN2: 100% vs. 97.1% vs. 71.4%; p = 0.001) and positive nodal status (pN0 vs. pN1+2: 100% vs. 86.3%; p = 0.009). On further analysis, it was found that 3 of 4 patients having contralateral neck failures had N2b disease. One patient with contralateral neck failure had N1 disease leading to a crude failure rate of 2.7% (1/37 patients). The histopathological feature of patients with contralateral neck failure were as follows: patient #1 (pT2N2b, PNI+, LVI+, moderately differentiated, clear margins, DOI 10 mm), patient #2 (pT4N1, PNI+, moderately differentiated, clear margins, DOI 6 mm), patient #3 (pT2N2b, moderately differentiated, clear margins, DOI 12 mm), and patient #4 (pT1N2b, well differentiated, clear margins, DOI 10 mm). All 4 patients had undergone a modified neck dissection. Statistically significant difference in ipsilateral nodal failure rates were found with higher nodal burden (pN0 vs. pN1 vs. pN2: 94.8% vs. 77.3% vs. 80.1%; p = 0.033) and positive nodal status (pN0 vs. pN1+2: 94.8% vs. 78.8%; p = 0.038). The crude distant failure rate was 4.3% (5/116). The 2-year DMFS was 95.4%.
6. Multivariate analysis
The prognostic factor significantly associated with poorer control rates, that is pN stage was further evaluated by Cox regression multivariate analysis. In the analysis of pN0 vs. pN+, p-value was found significant for OS (hazard ratio [HR] = 0.372; 95% confidence interval [CI], 0.16–0.85; p = 0.02) and DFS (HR = 0.356; 95% CI, 0.15–0.81; p = 0.04). Nodal stage N2 was associated with worst outcomes for OS, DFS, and LRC.
Discussion and Conclusion
This retrospective review aims to analyse prognostic factors and outcomes associated with the treatment of buccal mucosa cancers receiving ipsilateral radiotherapy in a tertiary cancer centre. Ghoshal et al. [16] reported 80% oral cancers presenting with stage III and IV. Our cohort had similar findings at 67% advanced cancers at presentation. The decision of need for ipsilateral or bilateral neck radiotherapy is generally arrived upon after assessing the clinicopathological features in the post-operative histopathology and the risk of nodal drainage to ipsilateral and contralateral lymph nodes [8]. The risk of nodal metastasis leading to neck failure varies among different sites of oral cavity in the range of 30%–40% [17]. For buccal mucosa, the risk ranges from 10% to 30% [18-20], while for other sites like tongue it is generally mentioned in the range of 15%–75% [21-24]. Buccal cancers have higher neck control rates as compared to sites like tongue, as reported by Liao et al. [24], 5-year neck control rate of 93% versus 86% (p = 0.0115) in a retrospective comparison of buccal and tongue cancers.
Several authors have previously reported on unilateral radiation therapy in well-lateralized oral cavity and oropharyngeal cancers [10,13,18,25] with excellent outcomes in terms of survival and contralateral neck control, but limited reports have been published addressing outcomes in cases of buccal cancers treated with unilateral irradiation. Publications by Vergeer et al. [13] and Cerezo et al. 18] have reported 5-year OS rates of 61% and 82.5%, respectively, in a combined cohort of oral cavity and oropharyngeal malignancies. Both these studies included a mixed bag of patients, and hence the outcomes cannot be directly applied to a site like buccal mucosa, which is generally well lateralized. One of the larger studies focusing on outcomes of combined modality treatment in buccal mucosa cancers was reported by Lin et al. [8], who reported outcomes of 145 cases, of which 125 were treated with ipsilateral irradiation. The 5-year OS was 55%. However, it included all types of buccal mucosa cancers, including those with extracapsular extension which accounted for 31.7% patients warranting concurrent chemoradiotherapy. So, the inclusion of high risk patients may have resulted in inferior outcomes compared to the cohort of patients in the previously mentioned studies. Another report by Habib et al. [26] addresses the results of unilateral face and neck treatment in 481 oral cavity cancers, but only 165 cases received combined modality treatment. The current report is one of the first study addressing the outcomes of unilateral irradiation in buccal mucosa cancers.
The incidence of various prognostic factors was comparable to that of other studies, PNI was present in 26.7% [27], while moderately differentiated tumors were around 48%. DeConde et al. [27] have reported 29% incidence of PNI and moderately differentiated tumors were 48%. Diaz et al. [22] and Pop et al. [28] have reported the timing of locoregional failure to be 12 months or before 24 months. While most of the recurrences tend to happen within the first 2 years [16], the incidence of recurrence in neck varies from 5%–10% for early cancers [13] to 25%–30% in advanced cases [22]. Our outcomes also corroborate with the literature with most failures (63.6%) happening within 24 months. The current study failed to show a predictive relationship between pT stage and overall TNM stage. This could be attributed possibly to the fact that, the patients with early stage tumors, i.e., pT1/2 tumors were associated with more number of other poor prognostic factors and also that is the reason they received radiotherapy. Nodal staging was associated with significantly poor outcomes in terms of OS, DFS, and LRC. Pathological node positive (pN+) disease status was associated with statistically significant differences in OS, DFS, LRC, and RC, although pN+ status didn’t influence LC in our study. No significant differences were found in OS with LVI, PNI or grade, although there was a trend towards significant decrement in OS with LVI+ disease and grade.
There is paucity of literature addressing CLNF following unilateral neck surgery and irradiation in buccal cancers. The incidence of CLNF varies according to the site of primary tumor. For oral cavity cancers, it is reported to be 0.9%–36% [29-32]. However, for anatomical site like buccal mucosa which has drainage largely to ipsilateral lymph nodal regions, have negligible rates of contralateral lymph node recurrence ranging from 0%–5.7% (Table 3). The chances of CLNF increase with T stage [29-31]. However, some other studies suggest no variation in CLNF with T stage [13,32]. Several other studies mention variation with grade of the tumor [26,31,33,34] while one study by Kowalski et al. [28] suggests no association of CLNF with differentiation status. Presence of nodes draining ipsilaterally entail a poor prognosis and increase the risk of CLNF [13,26,32-36]. Twenty-seven percent (13/48) cases with pN+ disease had locoregional failures in our study. Four out of 48 pN+ cases (8.3%) had CLNF in our cohort. Capote-Moreno et al. [33] have reported similar outcomes with 21.6% patients showing contralateral neck failures in patients presenting with pN+ disease and 6.4% contralateral neck failure rates in ipsilateral nodal disease. Table 3 shows studies assessing various prognostic factors which affect the rate of involvement of contralateral lymph node in buccal mucosa cancers.
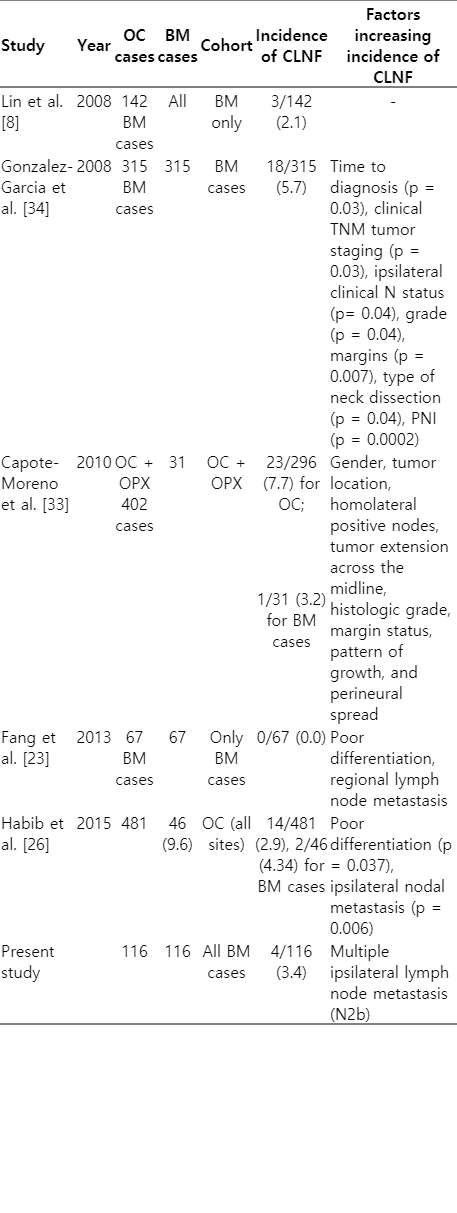
Studies depicting CLNF in buccal mucosa cancers and factors affecting it
Ipsilateral radiotherapy decreases doses to contralateral salivary gland, thereby decreasing incidence of xerostomia [35]. The ipsilateral fields also cause decrease rates of mucositis as lower volumes of oral mucosa is irradiated [36]. There is growing evidence in the literature that ipsilateral radiotherapy in oral cavity cancers is as good as bilateral radiotherapy, with better side effect profile [37]. The effectiveness of ipsilateral radiotherapy in a particular group of patients is because of low incidence of contralateral nodal involvement. In the previously published series by Lin et al. [8] which evaluated treatment outcomes in buccal mucosa cancers, it was opined by the authors that bilateral irradiation was given more to patients with N2 disease, but it conferred no significant benefit (p = 0.95) over unilateral radiotherapy in terms of LRC. Based on these facts, they recommend unilateral radiotherapy in cases with multiple lymph nodes.
Based on our results, we recommend that contralateral neck irradiation may be avoided safely in intermediate risk group of patients as per inclusion criteria of our study. We also recommend individualizing the balance between the risk of contralateral nodal failure and expected toxicity of bilateral irradiation while considering ipsilateral or bilateral irradiation in buccal mucosa cancers particularly in patients with multiple number or level of ipsilateral nodal involvement.
Certain limitations associated with this analysis have been enumerated. Firstly, the report is retrospective in nature. Secondly, we have reported the study with a median follow-up of 2 years, although it is worth considering that most of the failures happen within the first 2 years [16]. The above-mentioned limitations, however, highlight the importance of publishing single institutional data, which are eventually consolidated through meta-analysis. Moreover, this type of data is likely to come from retrospective studies only, thereby further highlighting the need to address this issue, so that we can exclude that cohort of patients from ipsilateral radiation which have high likelihood of failure, either locally or regionally, including ipsilateral and contralateral failures. Strength of the study includes a pure patient sample with homogenous uniform treatment, and to the best of our knowledge and as per the literature review the first such study addressing a ipsilateral radiotherapy in buccal mucosa cancers. This study will further add to the understanding of the pattern of failures and addresses the cohort of patients which might benefit the most by irradiation of the bilateral rather ipsilateral neck.
In conclusion, the incidence of contralateral recurrence in buccal mucosa cancer patients treated with primary surgery and adjuvant ipsilateral irradiation is low. It points to the fact that buccal mucosa carcinoma patients with intermediate risk factors can be spared of bilateral irradiation, without significantly affecting the OS and LRC rates. Patients with multiple pathologically involved nodes are at higher risk for developing contralateral regional recurrence as compared to node-negative disease.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.