Introduction
Positron emission tomography (PET)/computed tomography (CT) with 18F-fluorodeoxyglucose (FDG) is used extensively for staging and monitoring in patients with uterine cervical cancer [1]. Because of high glucose metabolism, FDG generally accumulates in malignant lesions. FDG uptake, however, is not specific for cancer cells and, therefore, sometimes results in false-positive conclusions for benign inflammatory lesions [2]. We report a case of uterine adenomyosis showing increased 18FDG uptake on PET/CT mimicking malignant tumor in a 44-year-old woman during concurrent chemoradiation therapy (CCRT) for uterine cervical cancer. However, the 18FDG uptake was completely resolved one month after completion of RT. Our case indicates that uterine adenomyosis in a premenopausal woman may result in false positive 18FDG-PET/CT findings. To our knowledge, false positive uterine 18FDG uptake in adenomyosis during CCRT for cervical cancer has not been previously described.
Case Report
A 44-year-old woman presented with a two-week history of painless abnormal vaginal bleeding and was referred to the gynecology department in August 2010. Upon pelvic examination, a 4-cm exophytic, cancerous lesion was identified in the uterine cervix that extended into the cervical canal. The right side of the parametrium was fixed. Punch biopsies were collected, and invasive squamous cell carcinoma of the cervix confirmed. There was no evidence of distant metastasis at that time. International Federation of Gynecology and Obstetrics (FIGO) stage IIB cervical cancer was diagnosed.
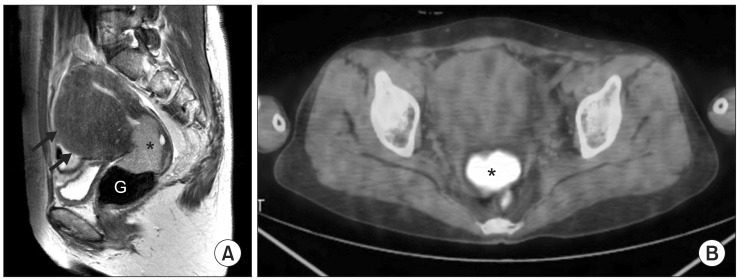
Magnetic resonance imaging (MRI) showed a 4.5-cm cervical tumor with direct invasion of the right parametrium and upper vagina. Multiple lymph node enlargements were also identified along the right external iliac and right retrocaval chain. In the uterus, multiple uterine myomas and an adenomyosis were noted (Fig. 1A). 18FDG-PET/CT examination was performed, demonstrating significant uptake in the uterine cervix mass, right external iliac and retrocaval lymph nodes (Fig. 1B).
The patient underwent CT scans for radiation therapy (RT) planning. The gross target volumes were defined as the lesions noted on the MRI and 18FDG-PET/CT. The clinical target volumes included the entire pelvis and the para-aortic area up to the upper body of the first lumbar spine. The major tumor and whole pelvis were treated over six weeks with 28 fractions of 50.4 Gy with anteroposterior/posteroanterior RT fields of 15-MV photons.
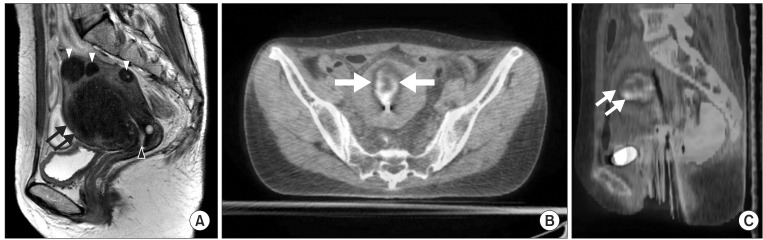
The regimen for CCRT consisted of six cycles of 5-fluorouracil (1,000 mg/m2 in a continuous infusion over 96 hours) and cisplatin (60 mg/m2) at three-week intervals. On interim MRI and PET/CT imaging for intracavitary radiotherapy (ICR) planning after the 23rd fraction of 4,140 cGy external radiotherapy, tumor size and 18FDG uptake in the cervix were markedly decreased. However, a new region of abnormal uptake appeared around a pre-existing adenomyosis in the anterior body of the uterus (Fig. 2).
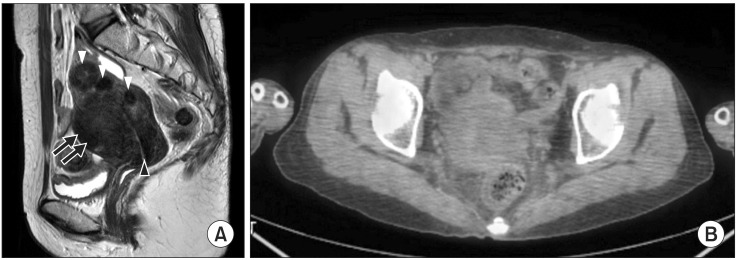
After external radiotherapy, PET/CT-guided high-dose ICR using an iridium-192 source was carried out with a reference tumor prescription of 24 Gy, three times a week in six fractions. One month after completion of RT, follow-up imaging was performed. There was no evidence of malignancy on either MRI or 18FDG-PET/CT. In addition, 18FDG uptake in the uterine anterior body was completely resolved (Fig. 3). The patient was premenopausal; however, menstruation did not occur after CCRT. Delayed toxicity related to RT was also reported.
Discussion and Conclusion
Adenomyosis is a common non-neoplastic gynecologic disease characterized by excessive migration of the endometrial glands and stroma from the basal layer of the endometrium into the myometrium [3]. The ectopic endometrium may be localized or diffusely distributed throughout the myometrium, leading to the formation of adenomyomas [4]. The diagnosis is usually based on histological findings in surgical specimens. MRI is a widely accepted method for achieving a valid pre-surgical diagnosis [5]. Some research has reported that postmenopausal patients with no known gynecologic malignancy had very mild FDG uptake [6]. Therefore, in postmenopausal women, all increased endometrial uptake is of clinical significance, and further investigation of the uterine pathology is advised.
However, in premenopausal women, endometrial uptake is related to the menstrual cycle and is highest during menses, followed by the level in the ovulation phase [5]. Endometrial FDG uptake during menstruation may be related to the peristaltic movements of the subendometrial myometrium that help to discharge menstrual blood [5]. The endometrial uptake in premenopausal patients using oral contraceptives resembles that in non-ovulating, non-menstruating premenopausal subjects [6], which is likely secondary to the effects of oral contraceptives including suppression of glands and atrophic introduction of the endometrium.
In our case, endometrial tissue in the myometrium showed new 18FDG uptake (standardized uptake values, 5.1) during CCRT that was not detected during the staging examination. The possibility of physiologic 18FDG endometrial uptake was suggested, but her normal endometrium did not exhibit significant uptake. Adenomyosis generally shows mild FDG uptake in premenopausal women, with increased uptake during menstruation and ovulation [7].
High uptake of 18FDG PET/CT during CCRT (external radiotherapy 4,140 cGy/23 fraction) in this case was assumed to have no association with the menstrual cycle as the patient reported no menstruation after the initiation of CCRT. Cole previously reported that permanent amenorrhea was induced after a single pelvic radiation dose of 4.5 Gy in 90% (70/78) of women aged 40 to 44 years, 96% (71/78) of women aged 45 to 49 years, and 100% (25/25) of women older than 49 years [8]. Considering that radiation might cause an immunologic reaction at the irradiated site, in addition to direct injury [8], this temporary abnormal uptake during CCRT may be related to certain inflammatory responses of adenomyosis due to radiation damage.
The utilization of 18FDG-PET/CT in the staging and assessment of cervical malignancies has been rapidly increasing in recent years. However, false-positive results have been reported with 18FDG-PET/CT in the uterus and are thought to be the results of physiologic and benign causes. Moreover, in patients with known cervical cancer, endometrial uptake may be increased even though no endometrial invasion or involvement is actually present [6]. Therefore, proper 18FDG-PET/CT image interpretation requires knowledge of physiologic and normal biodistributions of 18FDG throughout the body.
As exemplified in this case, the abnormalities seen on 18FDG-PET/CT must be compared to anatomic imaging results such as those of MRI, for further characterization as likely malignant or benign. We report this case because failure to recognize this kind of potential focal uptake on an 18FDG-PET/CT scan may lead to an erroneous interpretation and improper tumor volume contouring for image-guided radiation therapy.