Morphologic change of rectosigmoid colon using belly board and distended bladder protocol
Article information
Abstract
Purpose
This study investigates morphologic change of the rectosigmoid colon using a belly board in prone position and distended bladder in patients with rectal cancer. We evaluate the possibility of excluding the proximal margin of anastomosis from the radiation field by straightening the rectosigmoid colon.
Materials and Methods
Nineteen patients who received preoperative radiotherapy between 2006 and 2009 underwent simulation in a prone position (group A). These patients were compared to 19 patients treated using a belly board in prone position and a distended bladder protocol (group B). Rectosigmoid colon in the pelvic cavity was delineated on planning computed tomography (CT) images. A total dose of 45 Gy was planned for the whole pelvic field with superior margin of the sacral promontory. The volume and redundancy of rectosigmoid colon was assessed.
Results
Patients in group B had straighter rectosigmoid colons than those in group A (no redundancy; group A vs. group B, 10% vs. 42%; p = 0.03). The volume of rectosigmoid colon in the radiation field was significantly larger in group A (56.7 vs. 49.1 mL; p = 0.009). In dose volume histogram analysis, the mean irradiated volume was lower in patients in group B (V45 27.2 vs. 18.2 mL; p = 0.004). In Pearson correlation coefficient analysis, the in-field volume of rectosigmoid colon was significantly correlated with the bladder volume (R = 0.86, p = 0.003).
Conclusion
Use of a belly board and distended bladder protocol could contribute to exclusion of the proximal margin of anastomosis from the radiation field.
Introduction
Preoperative chemoradiotherapy (preop CRT) followed by surgery is a standard treatment for locally advanced rectal cancer. Most randomized prospective studies have reported the feasibility and safety of preop CRT [1234]. However, some patients treated with preop CRT experience postoperative morbidity [5]. Anastomotic leakage (A-leak) is one of the most severe complications after surgery. The risk factors for A-leak after surgery have been evaluated, but remain controversial as the findings are often inconclusive. Several studies identified preop CRT as a risk factor for A-leak and some surgeons are therefore reluctant to perform preoperative radiotherapy (RT). Irradiated bowel shows different pathologic characteristics compared with non-irradiated bowel. Radiation-related reactions include inflammatory infiltrations, erosions, and decreased mucus secretion [6]. Such reactions create complications for surgeons when manipulating the bowel for anastomotic surgery.
A-leak seems to be more likely in patients who receive a higher radiation dose and have a larger irradiated volume of potential anastomotic site. Radiation to both sides of the anastomosis reduces the anastomotic strength. However, several experimental studies have reported that if only one segment of the anastomosis has been irradiated, the anastomosis can be safely constructed without adverse effects on wound healing [789]. By constructing an anastomosis consisting of an irradiated and a non-irradiated colon segment, proliferation of fibroblasts and epithelialization are improved compared to an anastomosis consisting of two irradiated sides [7]. Therefore, efforts should be made to exclude one segment of anastomosis from the radiation field to reduce A-leak.
Coloanal or ultralow colorectal anastomosis has commonly been performed in patients with rectal cancer. The level of anastomosis is affected by the location and extent of the tumor and blood supply of the sigmoid colon and rectum. The proximal margin of anastomosis is usually in the sigmoid colon, which is often included in the radiation field because of anatomical redundancy. By straightening the rectosigmoid colon, it may be possible to exclude the proximal margin of the anastomosis from the radiation field, thereby reducing the irradiated volume and lowering the rate of postoperative complications.
Since 2009, a belly board in prone position and distended bladder protocol has been used in radiotherapy for rectal cancer in Yonsei Cancer Center to reduce the irradiated volume of the small bowel. In this study, we investigate morphologic changes of the rectosigmoid colon using our protocol. We also evaluate the possibility of excluding the proximal margin of anastomosis from the radiation field by straightening the rectosigmoid colon.
Materials and Methods
1. Patient selection
Nineteen patients with adenocarcinoma of the rectum who received pelvic RT between 2006 and 2009 with preoperative intent were analyzed. Patients treated during this period had a treatment planning computed tomography (CT) scan in prone position only (group A). Each patient was individually matched by sex, age, and body mass index (BMI) with other 19 patients who were treated between September 2010 and May 2011 (group B). Since 2009, a belly board has been used for patients with rectal cancer in Yonsei Cancer Center to displace the small bowel from the radiation field. In addition, all patients in group B were instructed in bladder distension techniques.
2. Distended bladder protocol
Patients in group B were instructed to fill their bladder before simulation in our institutional protocol [10]. They were asked to drink an unspecified volume of water because there were wide variations in the ability of patients to drink water and retain urine. Instead, patients were instructed at the first visit to voluntarily regulate their volume of drinking water. The goal of these instructions was to maintain a similar volume during the treatment course, therefore if the volume of the bladder was less than 200 mL the patient was asked to drink a cup of water (100-150 mL) and wait until the bladder was distended to more than 200 mL. Two trained doctors measured the volume of the bladder before CT simulation using a portable automated ultrasonic bladder scanner (BioCon-700; Mcube Technology, Seoul, Korea). In the entire course of treatment, the patient's bladder was filled as an initial protocol and scanned weekly, immediately before RT. The measured volume was disclosed to the patients and recorded in their medical chart. During simulation and treatment, patients were in a prone position using a bladder compression device and belly board designed by our institution [1112].
3. Rectosigmoid colon delineation
Because the diameter of the rectosigmoid colon is significantly affected by bowel gas and/or feces, we assumed that the rectosigmoid colon is a cylinder of 2-cm diameter to calibrate differences in diameter. The rectosigmoid colon was delineated by a 2-cm diameter circle at each axial cut of the planning CT images from the level of the levator ani muscles to the level of the sacral promontory (Fig. 1). Thus, by measuring the volume of the cylinder, we could predict the volume of the rectosigmoid colon in the pelvic cavity.
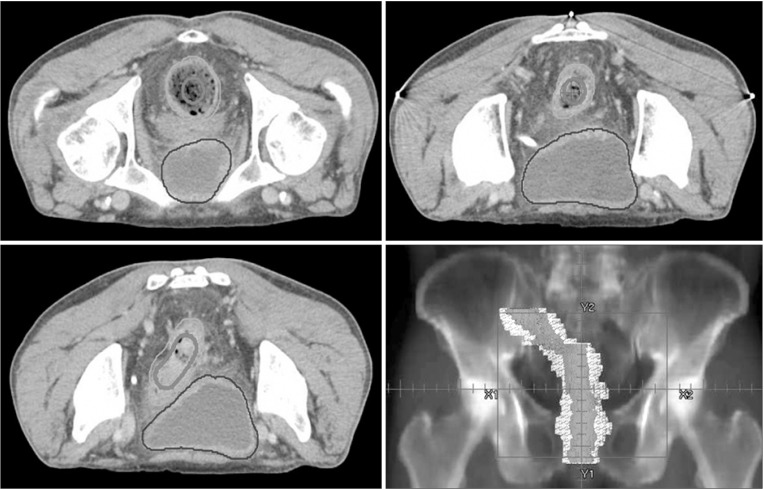
Delineation of rectosigmoid colon on simulation computed tomography (orange, actual rectosigmoid colon delineated on axial slice; pink, modified delineation as a cylinder with 2-cm diameter).
One radiation oncologist contoured the bladder and rectosigmoid colon on the simulation CT image and calculated their volumes. The rectosigmoid colon was assessed for redundancy by relating the morphologic changes on the digitally reconstructed radiography (DRR) images. Patients were subsequently divided into four groups: no redundancy, 1 redundancy, 2 redundancies, and 3 or more redundancies (Fig. 2).

Assessment of redundancy by relating morphologic changes on the digitally reconstructed radiography images. Patients were subsequently divided into four groups: (A) no redundancy, (B) 1 redundancy, (C) 2 redundancies, (D) ≥3 redundancies.
4. RT planning and DVH parameters
In all cases, the radiation treatment portals encompassed the entire pelvis through a posterior portal and right and left lateral treatment portals. The superior border of the radiation field was placed at the level of the L5-S1 interspace. The inferior border was at the bottom of the obturator foramen. Both lateral margins of the posterior portal were 1 cm from the pelvic rim. The anterior aspect of the right and left lateral field was placed 2 cm in front of the most anterior aspect of the sacral promontory. Posteriorly, the entire sacrum was included 0.5 cm from the most posterior aspect of the coccyx.
A 6-MV posterior photon beam and 10-MV photon lateral beams were used. The posterior portal delivered 40% of the prescribed dose and each lateral portal delivered 30% of the prescribed dose. To calculate the dose of the rectosigmoid colon, excluding the effect of additional boost RT, the treatment plan was irradiation of the whole pelvic field with a total dose of 45 Gy with 1.8 Gy per fraction.
We compared the volume of the rectosigmoid colon and the number of redundancies of the rectosigmoid colon in the pelvic cavity below the sacral promontory level by DRR imaging. The volume of the entire bladder was also evaluated for the two groups. A dose volume histogram (DVH) of the rectosigmoid colon was generated for the RT field. The volume of rectosigmoid colon receiving each dose between 5 and 45 Gy was recorded at 5-Gy intervals.
5. Data analysis and statistics
Statistical analysis was performed using SPSS statistics ver. 19.0 (IBM SPSS Inc., Armonk, NY, USA). Patient characteristics of the two groups were analyzed using the chi-square test. Redundancy and volume of rectosigmoid colon in the pelvic cavity were compared using Wilcoxon signed-rank test. Differences in mean rectosigmoid colon volume irradiated to each 5-Gy dose level from 5 to 45 Gy were assessed using the t-test for equality of means. Pearson correlation coefficient was used to evaluate the relationship between the volume of the bladder and that of the rectosigmoid colon.
A-leak after surgery was assessed by retrospectively reviewing the medical records of all patients. Symptomatic A-leak was defined as clinically apparent leakage (gas, pus, or fecal discharge from the pelvic drain, or peritonitis) or extravasation of endoluminally administered water-soluble contrast on imaging study.
Results
1. Patient characteristics
Table 1 summarizes the characteristics of patients in the two groups. Median age of all patients was 60 years and median BMI was 22.4. Patients in both groups were well matched by age, sex, and BMI. The extent of disease was similar in the two groups. All patients were clinical T3 or T4 stage, and 82% were clinical T3 stage. Eighty-seven percent of patients had clinically lymph node-positive disease.
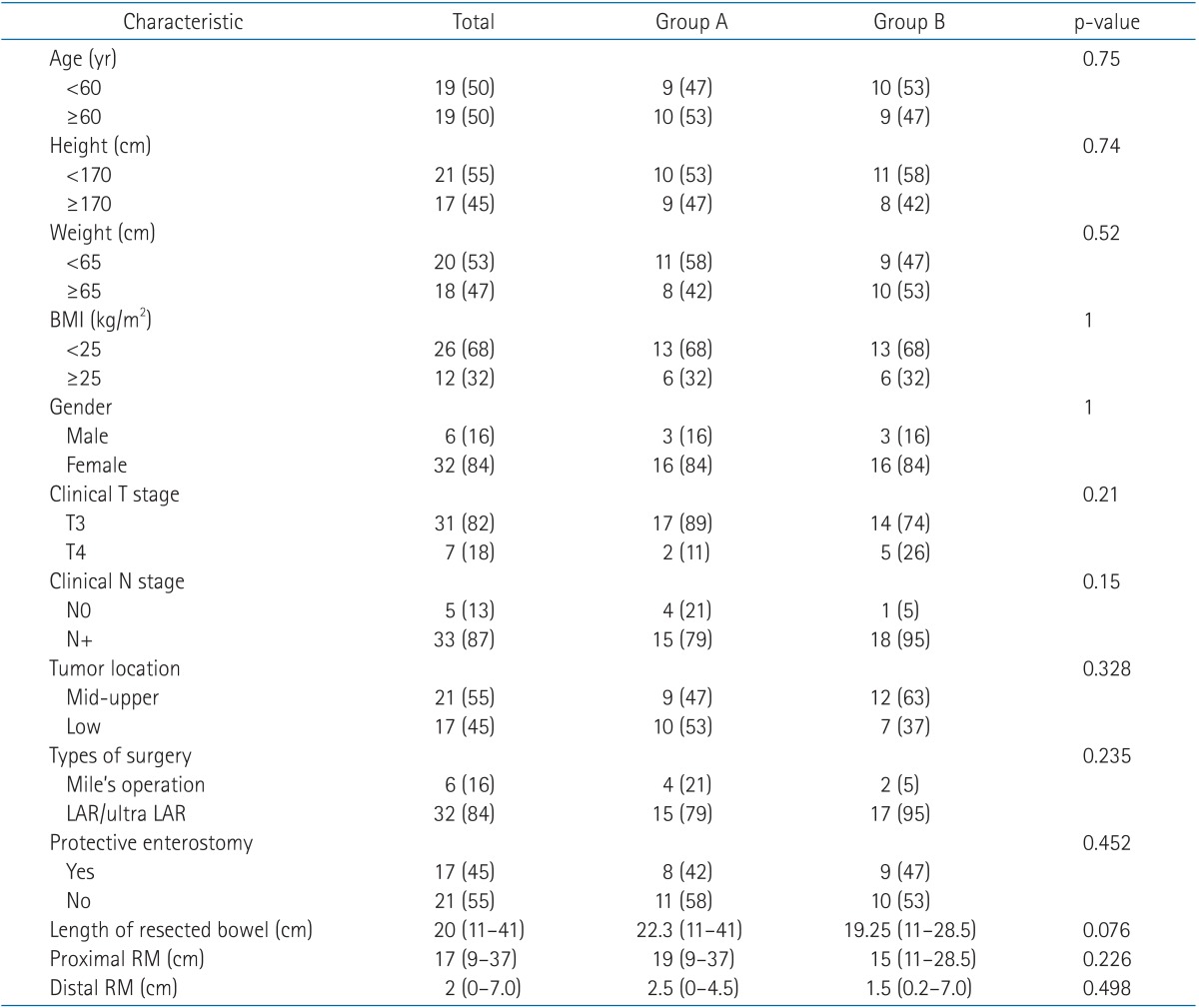
Patients' characteristics
In general, the degree of proximal resection margin was determined by the surgeon. After ligating the inferior mesenteric vessels, the rectum was oversewn or stapled below the tumor and a proximal resection margin greater than 5 cm was recommended. Either the sigmoid or descending colon was used for reconstruction. The length of resected bowel was similar between both groups. The median length of resected bowel was 22 cm for lower rectal cancer (location of lower margin <5 cm from anal verge) and 19 cm for mid-upper rectal cancer. The proximal and distal margin status of surgical specimens showed no significant difference between the two groups.
2. Morphologic and DVH analysis of rectosigmoid colon
A greater number of patients in group B, who were treated using belly board and distended bladder protocol, had a visually straightened rectosigmoid colon compared with group A (no redundancy; group A vs. group B, 10% vs. 42%; p = 0.03). Table 2 shows comparisons of morphology as determined by the redundancy and volume of the rectosigmoid colon in the pelvic cavity. The volume of the rectosigmoid colon was significantly larger in group A (56.7 vs. 49.1 mL; p = 0.009). The number of redundancies was relatively high in group A compared with group B, but did not show statistical significance (p = 0.06). Fig. 3 shows the mean irradiated volumes of rectosigmoid colon in both groups per 5-Gy dose increment. The volume of irradiated rectosigmoid colon was significantly lower for patients in group B at all dose levels, and this difference was more significant at a higher dose (V45; 27.2 vs. 18.2 mL; p = 0.004).
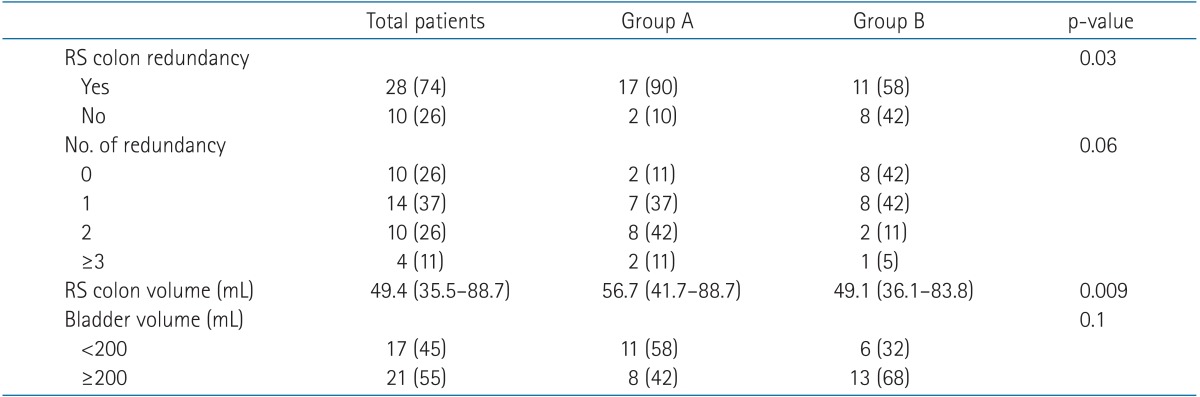
Analysis of rectosigmoid (RS) colon and bladder volume

Mean irradiated volumes of rectosigmoid colon per 5-Gy dose increment for both groups.
A larger proportion of patients in group B (68%) than in group A (42%) had distended bladder (≥200 mL), but this did not show statistical significance (p = 0.1) (Table 2). In Pearson correlation coefficient analysis, the volume of rectosigmoid colon in the radiation field was significantly correlated with the volume of the bladder. A distended bladder was more likely to make the rectosigmoid colon straight (R = 0.86, p = 0.003) (Fig. 4).
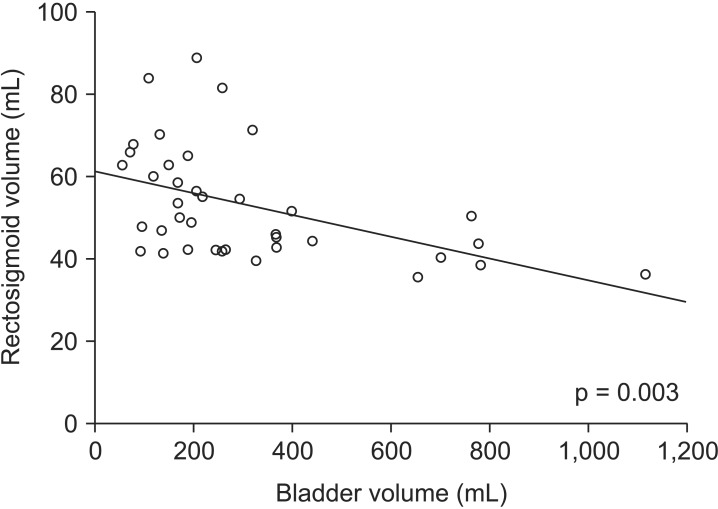
Pearson correlation coefficient analysis of the volume of rectosigmoid colon and the volume of bladder.
3. Anastomotic leakage
Three of 38 patients experienced A-leak: 2 in group A and 1 in group B. The length of resected bowel was similar among these patients and the location of the tumor was also comparable (Table 3). One patient in group B (patient no. 3) had a relatively large volume of rectosigmoid colon (83.8 mL) and three redundancies in the pelvic cavity despite being treated with a belly board. Although this patient was instructed to fill the bladder before the CT scan, the total bladder volume was only 110 mL. All of these patients were treated with diverting loop ileostomy and managed by primary repair 6-18 months later.

Characteristics of patients who experienced postoperative anastomotic leakage after preoperative chemoradiotherapy and surgery
Discussion and Conclusion
Radiation volume and dose to normal bowel, which correlate with radiation-related toxicities, are critical parameters, especially in the sigmoid colon, which is used for anastomosis after rectal radiation therapy and resection. As part of our efforts to reduce small bowel toxicities, we previously reported that our institutional policy including 1) prone position, 2) belly board with bladder compression device, and 3) full bladder instruction with intensive feedback using an ultrasonic bladder scanner could play an important role in reducing radiation exposure to the small bowel [101112]. The objective of the current study was to validate the hypothesis that our institutional protocol could straighten the rectosigmoid colon, thus reducing radiation exposure to the potential anastomotic site. To test this, we delineated the rectosigmoid colon of 38 patients with rectal cancer. Nineteen patients treated between 2006 and 2009 had a treatment-planning CT scan in the prone position only (group A), whereas 19 patients treated between 2010 and 2011 underwent simulation using a belly board in prone position and distended bladder protocol (group B). We found that patients in group B had a higher frequency of a visually straightened rectosigmoid colon than patients in group A (no redundancy; group A vs. group B, 10% vs. 42%; p = 0.03). Furthermore, in DVH analysis the mean irradiated volume at all dose levels between 5 Gy and 45 Gy was also lower for patients in group B, and this reduction was more prominent at a higher dose (V45; 27.2 vs. 18.2 mL; p = 0.004). These findings imply that the belly board and distended bladder protocol affects the morphology of the rectosigmoid colon such the proximal segment of potential anastomosis could be excluded from the RT field, thus supporting our hypothesis.
The pathological effects of radiation in the intestine of humans and experimental animal models are well described [13141516]. During the first few weeks of radiation, acute injury is seen in the rapidly dividing mucosal epithelial cells. Later, progressive changes in deeper fibrovascular tissue are identified as chronic radiation injury. These radiation-induced changes in intestinal tissue can affect the anastomotic healing [17].
Whether these pathologic changes increase the rate of A-leak remains controversial as the results of studies to date are not conclusive and potential fear of A-leak is a major reason for avoiding preop CRT. In a prospective randomized trial comparing preop CRT and postop CRT, the overall incidence of A-leak was not significantly different between the two groups (11% vs. 12%; p = 0.77) [18]. In contrast, several studies have reported an influence of preop CRT on A-leak. One case control study using the Swedish registry (1995-2000) concluded that preop CRT was the most important risk factor for A-leak (odds ratio = 1.34) [19]. In another retrospective study, Lee et al. [20] revealed that preop CRT was associated with an increased risk of A-leak with a relative risk of 2.86 (p = 0.003). Faced with these negative results, strategies to reduce the risk of A-leak should be considered when planning radiotherapy.
In general, the belly board and the distended bladder protocol are used in an attempt to reduce the irradiated volume of the small bowel during radiotherapy for patients with rectal cancer. Various studies have demonstrated the effectiveness of these methods for displacing the small bowel outside the pelvis. Koelbl et al. [21] reported the effect of the belly board in rectal cancer patients treated with postoperative RT. They reported that the irradiated volume of the small bowel was reduced by 54% in the prone position combined with belly board, compared with the prone position only. Other studies reported that the distended bladder protocol further reduced the irradiated small bowel volume compared with the prone position alone [2223]. Based on these results, the belly board and distended bladder protocol has been used for pelvic irradiation in our institution since 2009. In our study, these methods reduced radiation exposure of potential anastomotic site by straightening the rectosigmoid colon (no redundancy 10% vs. 42%, p= 0.03; V45 27.2 vs. 18.2 mL, p = 0.004). In particular, the volume of the bladder was significantly associated with the irradiated volume of the rectosigmoid colon (R = 0.86, p = 0.003) (Fig. 4). A 2 × 2 study with belly board and distended bladder protocol as the independent variables is needed to confirm this result.
Three patients experienced A-leak: 2 in group A and 1 in group B. One patient in group A with A-leak had a distended bladder (bladder volume = 259.1 mL) and a relatively straightened rectosigmoid colon. Although the anastomotic site was exposed to a low dose of radiation, there might be other risk factors for A-leak in this patient. Studies evaluating the risk factors for A-leak after surgery have shown that the level of the tumor, advanced stage, male gender, smoking, perioperative bleeding, and pre-existing disorders are factors related to A-leak [242526]. As multiple factors are involved in A-leak it is difficult to identify the independent effect of this protocol on the reduced risk of A-leak in the clinical setting.
There are several limitations in this study. First, given the small number of patients enrolled in this study and few cases of A-leak, we cannot conclude that these combined methods reduce the crude rate of A-leak. Because of the low incidence of A-leak requiring reoperation [27], it is difficult to demonstrate the association between these methods and A-leak without a large randomized study. It seems better to investigate the subjective feelings of surgeons when they manipulate previously irradiated bowel using a questionnaire. Second, the level of anastomosis was not considered in the preoperative evaluation. We planned to treat all of the patients in this study with the same radiation field and did not consider the location and size of tumor or the shape and position variations of the rectum between the patients. These weaknesses should be taken into consideration when interpreting our results.
Overall, in the present study the number of the patients with a straightened rectosigmoid colon was increased by 30% points when using the belly board and distended protocol. This could contribute to exclusion of the proximal margin of anastomosis from the radiation field and reduce the incidence of A-leak.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.