Recent trends in intensity-modulated radiation therapy use in Korea
Article information

Abstract
Purpose
We aimed to analyze the trend in intensity-modulated radiation therapy (IMRT) use in Korea from 2011 to 2018.
Materials and Methods
We collected data from the Health and Insurance Review and Assessment Service (HIRA) big data based on the National Health Insurance Service claims and reimbursements records using primary treatment planning codes (HD 041) for IMRT from 2011 to 2018. We analyzed the changing patterns in clinical application to specific tumor sites and regional differences in IMRT utilization.
Results
The use of IMRT has exhibited an 18-fold steep rise from 1,921 patients in 2011 to 34,759 in 2018. With regard to IMRT in 2018, 70% of patients (24,248/34,759) were treated in metropolitan areas (Seoul, Incheon, and Gyeonggi Province). IMRT was most commonly used to treat breast, lung, and prostate cancers in 2018. Among these, the use of IMRT for breast cancer shows the most remarkable increase from 2016 when the National Health Insurance began to cover IMRT for all solid tumors.
Conclusion
The use of IMRT is steadily increasing to treat cancer and is concentrated in metropolitan areas.
Introduction
In 2016, there were 203,129 new cancers in Korea except thyroid cancer, with the highest incidence in the order of stomach, colon, lung, breast and liver cancer. For men, the incidence rate of gastric cancer, colorectal cancer, and liver cancer has decreased, but prostate cancer increased steadily by 13% until 2009, but no longer increasing. In women, stomach cancer, colon cancer, liver cancer and cervical cancer are continuously decreasing, but breast cancer is steadily increasing [1].
To date, radiation therapy technology has steadily improved to reduce adjacent normal organ side effects and improve therapeutic effects in tumors. Radiation therapy has evolved from conventional two-dimensional therapy to three-dimensional conformal therapy (3D-CRT). Recently, radiotherapy technologies using intensity-modulated radiation therapy (IMRT) have been applied in most cancers. The use of IMRT to treat cancer is steadily increasing in Korea [2,3]. According to a recent report based on the big data of the Health and Insurance Review and Assessment Service (HIRA), IMRT was the second-most common radiotherapy modality following 3D-CRT, and the IMRT utilization rate in Korea was 23% in 2016 [2].
Until now, there have been few reports of IMRT use since the first implementation of IMRT in 2001 in Korea [2-4]. Moreover, there has been no report regarding the utilization of IMRT for specific cancer sites. Herein, we analyzed the current status of and changing patterns in IMRT use for specific cancer sites from 2011 to 2018.
Materials and Methods
We collected data from the HIRA based on the National Health Insurance Service claims and reimbursements records using primary treatment planning codes for IMRT (HD 041) from 2011 to 2018 [5]. The total amount of IMRT use was tallied based on the year of the insurance audit of the HIRA data. We analyzed changing patterns in clinical implementation according to the cancer site by year. We also investigated IMRT utilization by administrative district in 2018. Additionally, we used the status of radiotherapy facilities and machines at the end of 2018 [6].
Results
The total numbers of patients who received IMRT in 2011, 2013, 2015, and 2018 were 1,921, 5,992, 9,091, and 34,759, respectively (Table 1). The use of IMRT has exhibited an 18.6-fold steep rise from 2011 to 2018. Three cancers most frequently treated with IMRT in 2011 were head and neck, prostate, and central nervous system cancers, but in 2018, these changed to breast, lung, and prostate cancers. In 2018, compared to 2011, IMRT for breast cancer increased 148.3-fold in 2018, and the frequencies of IMRT in lung, hepatobiliary, and gastrointestinal cancers increased 37.8-, 34.2-, and 30.5-fold, respectively. Since the application of IMRT health insurance coverage in 2015, IMRT use increased dramatically in 2016 for most cancers (Fig. 1).
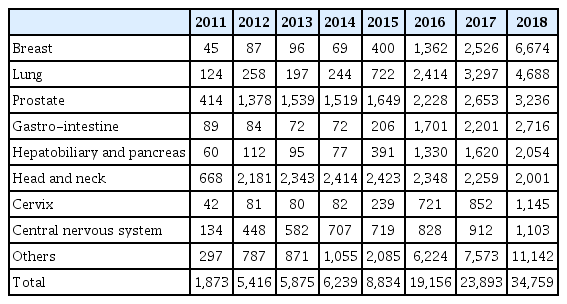
Number of patients who received primary treatment planning for IMRT by cancer site from 2011 to 2018
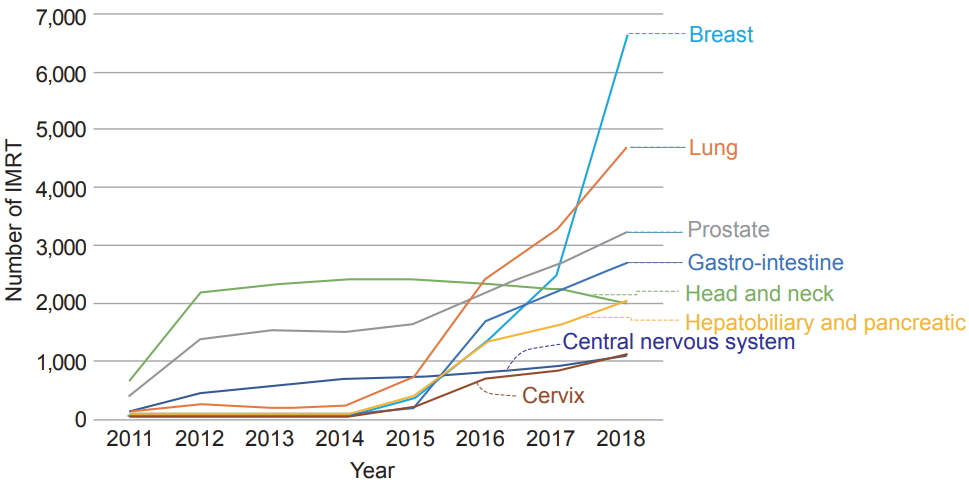
Use of intensity-modulated radiation therapy (IMRT) showed a remarkable increase from 2016 since the National Health Insurance expanded reimbursement for IMRT to include all solid tumors in 2015.
In 2018, 70% of new patients who received IMRT (24,248/34,759) were treated in metropolitan area such as Seoul, Incheon, and Gyeonggi areas. However, only 6.7% of patients received IMRT in areas that were not metropolitan, such as Gangwon, Chungbuk, Jeonbuk, and Jeju. In 2018, there were 91 radiation treatment facilities and 205 radiation treatment machines nationwide [6]. In 2018, the average number of IMRT patients administered per facility was 382.0, and the average number of IMRT patients administered per machine was 169.6 (Table 2). In Seoul, Incheon, and Gyeonggi areas, the number of IMRT patients administered per radiation therapy facility was 499.9, which was higher than the average, and the number of IMRT patients administered per machine was 190.2, which was also higher than the average. In areas that were not metropolitan, such as Gangwon, Chungbuk, Jeonbuk, and Jeju, the number of IMRTs administered per radiation therapy facility was 298.1, which was lower than the average, but the number of IMRT patients administered per machine was 174.5, which was slightly higher than the average.

Number of IMRT patients administered per radiation facility and machine per year according to area in 2018
Discussion and Conclusion
The use of radiotherapy in cancer patients has increased steadily from 25% in 2011 to 30% in 2015, and the use of IMRT is also rapidly increasing in Korea [2,3]. The current study showed that IMRT use has been increasing rapidly, showing an 18-fold steep rise from 1,921 patients in 2011 to 34,759 in 2018. Since IMRT was first performed in 2001 in Korea, implementation of IMRT has been partially covered by national health insurance for specific cancer sites (head and neck, brain, prostate, spinal cancers and re-irradiation cases) from 2011, and since July 2015, the coverage has expanded to include almost all cancers [4]. An abrupt increase from 2015, despite some controversy regarding the cost-effectiveness of IMRT, larger skin dose, and risk of radiation-induced secondary cancers, may have been due to the health insurance coverage and recent advancement in therapeutic machines for IMRT [2,3,7].
The current study showed that the three cancers most frequently treated with IMRT in 2011 were head and neck, prostate, and central nervous system cancers, but in 2018, these were breast, lung, and prostate cancers (Table 1). Among these, the use of IMRT for breast cancer showed the most remarkable increase. In Korea, the use of IMRT to treat breast cancer is steadily increasing to spare organs at risk, particularly the heart, in patients with left breast cancer and for hypofractionated whole-breast irradiation since 2015. According to the UK IMRT survey report in 2008, there is considerable variety in the definition of IMRT for breast cancer, with some studies using an inverse-planned technique with multiple gantry angles and others using so-called simple IMRT, consisting of a forward-planned field-within-field technique. This report showed that for breast cancer, forward-planned IMRT is prominently used instead of inverse-planned IMRT (5,517 vs. 56 patients) [8]. Despite the demonstrated benefit of modulating the intensity of the treatment field, there remains uncertainty regarding when the less expensive simple IMRT or 3D-CRT may be adequate and when the more resource-intensive, inverse-planned, high-cost IMRT is needed. In its ‘Choosing Wisely’ campaign, the American Society for Radiation Oncology (ASTRO) recommended that IMRT should not be routinely used to deliver whole-breast radiation as part of breast conservation therapy. Although IMRT may be beneficial in selected cases involving unusual anatomy, no studies have yet demonstrated that its routine use provides a significant clinical advantage [9]. According to the 2018 ASTRO evidence-based guideline for the whole breast radiation therapy, three-dimensional conformal treatment planning (3D-CRT) with a ‘field-in-field’ technique is strongly recommended as the initial treatment planning approach with 100% consensus, However, the guideline comments nothing about the role of IMRT [10].
IMRT utilization is increasing worldwide; however, there is a difference in the use of IMRT across individual treatment centers and by country [8,11]. Shumway et al. [11] reported a 4-fold variation in IMRT use among centers across the State of Michigan ranging from 23% in the lowest-use center to 96% in the highest-use center in 2012. The utilization rate of IMRT in radiation therapy in Japan was 15% in 2017, while it was 23% in Korea in 2016 [2,12]. In Japan, IMRT is only reimbursed by the national health insurance system when the following personnel are present: (1) two full-time radiation oncologists and a radiotherapy technician, each with more than 5 years of radiotherapy experience; and (2) an individual responsible solely for precision control of the radiotherapy devices, irradiation plan verification, and assistance with the irradiation plan (e.g., a radiotherapy or other technician) [13]. According to the Japanese Society for Radiation Oncology database report of 2018, IMRT was mostly used to treat prostate, head and neck, and central nerve system tumors in Japan [14]. On the other hand, in Korea, IMRT was most commonly used to treat breast, lung, and prostate cancers in 2018.
With regard to IMRT in 2018, 70% of new patients (24,248/34,759) were treated in metropolitan areas. The main reason for the need for medical travel to metropolitan areas among patients receiving radiotherapy was the concentration of facilities in the capital area and Korea’s advanced public transport system, including the high-speed railway line [15].
Our study has several limitations. The current study only included data of the insured patients for primary treatment planning for IMRT, excluding data of secondary planning for boost treatment, and the number of uninsured or foreign patients could not be recorded. Therefore, the actual number of patients who received IMRT is expected to be higher than the reported number. Despite these limitations, we think that this study provides the latest trends in the use of IMRT for specific cancer sites. In conclusion, the use of IMRT has been steadily increasing to treat cancer since 2011 and shows a metropolitan area concentration. Currently, IMRT is most commonly used to treat breast, lung, and prostate cancers.
In summary, it is necessary to redefine the clinical application of IMRT on the basis of prospective clinical studies that can prove clinical benefits of IMRT over 3D-CRT in the treatment of cancer patients. In addition, reviewing the cost-benefits will help to establish the basis for the clinical application of IMRT.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
We are grateful to the Health and Insurance Review and Assessment Service for providing valuable information.