Prospective evaluation of fiducial marker placement quality and toxicity in liver CyberKnife stereotactic body radiotherapy
Article information

Abstract
Background
Evaluate morbidities and “quality” of fiducial marker placement in primary liver tumours (hepatocellular carcinoma [HCC]) for CyberKnife.
Materials and Methods
Thirty-six HCC with portal vein thrombosis (PVT) were evaluated for “quality” of fiducial placement, placement time, pain score, complications, recovery time and factors influencing placement.
Results
One hundred eight fiducials were placed in 36 patients. Fiducial placement radiation oncologist score was “good” in 24 (67%), “fair” in 4 (11%), and “poor” in 3(8%) patients. Concordance with radiologist score in “poor”, “fair”, and “good” score was 2/2 (100%), 4/5 (80%), and 24/27 (89%), respectively (p=0.001). Child-Pugh score (p=0.080), performance status (PS) (p=0.014) and accrued during “learning curve” (p=0.013) affected placement score. Mean placement time (p=0.055), recovery time (p=0.025) was longer and higher major complications (p=0.009) with poor PS. Liver segment involved (p=0.484) and the Barcelona Clinic Liver Cancer (BCLC) stage did not influence placement score. “Good” placement score was 30% in first cohort whereas 93% in last cohort (p=0.023). Time for placement was 42.2 and 14.3 minutes, respectively (p=0.069). Post-fiducial pain score 0–1 in 26 patients (72%) and pain score 3–4 was in 2 (6%). Five patients (14%) admitted in “day-care” (2 mild pneumothorax, 3 pain). Mortality in 1 patient (3%) admitted for hemothorax.
Conclusion
Fiducial placement is safe and in experienced hands, “quality” of placement is “good” in majority. Major complications and admission after fiducial placement are rare. Complications, fiducial placement time, recovery time is more during the “learning curve”. Poor Child-Pugh score, extensive liver involvement, poor PS have higher probability of complications.
Introduction
Fiducial placement in liver tumours (hepatocellular carcinoma [HCC]) for robotic radiosurgery (CyberKnife) treatment is considered crucial step of treatment and also associated with morbidities [1]. In fact, fiducial placement is considered essential in both robotic radiosurgery (CyberKnife) and linac-based stereotactic body radiotherapy (SBRT) treatment. Fiducial markers for SBRT are generally introduced under percutaneous ultrasound or computed tomography (CT) guidance [2-4]. However, fiducial placement has it’s own issues and need to be addressed [5]. It leads to a delay in treatment. Many clinicians will impose up to a 1-week delay from fiducial placement to treatment planning in order to allow the markers to “settle” [6]. The fiducial placement procedure is also associated with potential risks and complications like pain, vasovagal attack, pneumothorax, hemothorax, perforation of non-target organs, bile peritonitis, infection, hemobilia, neuralgia, and tumor seeding [7,8]. “Ideal” fiducial placement means appropriately placed fiducials, neither too close nor too far from each other and close to the target. Apart from these placement related parameters, clinical parameters such as time for placement, recovery time, pain score after placement, are also critical [9]. “Quality” of placement is a combination of mechanical parameters as per fiducial placement and also clinical parameters related to the placement. Unfortunately, though there are specifications for an “ideal” placement of fiducials, there is no published parameter for “quality” of fiducial placement.
The literature on fiducial related complications and migration related parameters from Indian subcontinent is very scarce [10]. Compliance, acceptability and pain related issues may not be similar in the Indian population as observed in Western population [10]. There is no well-known prospective study looking into the actual rate of fiducial migration, accuracy of fiducial placement and its utility in treatment planning, pain score and procedure related parameters. There are also no standard guidelines for the amount of fiducial migration expected and hence the time required to start the treatment and this needs further evaluation. Our present prospective study is to evaluate the feasibility and accuracy of fiducial placement under image guidance and to evaluate the fiducial placement score, pain score, fiducial placement related complications and impact of fiducial placement on planning and treatment. The migration within liver during treatment (intra-treatment migration) related parameters were analyzed in separate manuscript due to space constraint.
Materials and Methods
Between one calendar year (Mar 2017–Mar 2018), 108 fiducial placements done in 36 primary liver tumours (HCC) and were accrued in the present Amrita Institute of Medical Science Institutional Ethical & Scientific Committee approved prospective observational study for robotic radiosurgery treatment (No. AIMS-2018 ONCO-124). Patients were accrued after obtaining consent in native language. All these patients were radiologically diagnosed HCC, have preserved liver function (bilirubin <4 mg/dL, platelet >75,000, international normalized ratio [INR] <2) and good performance status (PS 0–1 or early PS 2). All the patients underwent three specified fiducials place in the liver under either CT scan or ultrasound-guided. Fiducials were placed by radiologist with an ideal situation where the fiducials will be in equidistance from each other (max distance 5 cm and min distance 2 cm) and the angles between the fiducials are specified. Quality of fiducial placement as per the radiologist and treating radiation oncologist were assessed by institution defined parameters (Table 1). Placement time, pain score, complications, recovery time and factors influencing fiducial placement were analyzed. Demographic profiles of the patients are in Table 2.
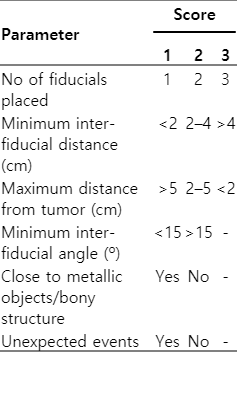
Fiducial placement accuracy scoring and grading system

Demographic profile of HCC patients underwent fiducial placement (n = 108)
1. Image guided fiducial placement and simulation
Fiducial placement was done under computed tomographic (SOMATOM Emotion 16 slice CT; Siemens, Erlangen, Germany) or ultrasonographic (Philips iU22 ultrasound; Philips Medical System, Cleveland, OH, USA) guidance under sterile conditions by an interventional radiologist (SG) in the presence of radiation oncologist (DD) to guide the placement of the fiducials. Three gold fiducials were inserted percutaneously under image guidance using a cylindrical 20-cm long 18-gauge puncture needle with a preloaded fiducial marker [11,12]. Each fiducial is a cylinder made from 99% pure gold with whorl on the surface. It weighs 17 gm and has a size of 1.2 mm × 5.0 mm (GF1521 gold fiducial marker; IZI Medical, Owings Mills, MD, USA). The accuracy of fiducial placement was scored by the interventional radiologist and the radiation oncologist independently based on the fiducial placement accuracy scoring system looking into parameters like inter-fiducial distance, inter-fiducial angle, distance from the centre of the tumor and any gross displacement or complications (Table 1). Score is done by number of fiducials, minimum and maximum distance between fiducials, close to bony structure and any unexpected events. Score of 14–15 is considered very good, 11–13 is good, 8–10 is fair, and 6–7 is poor.
Post procedure pain scoring was done using visual analog pain scale and any complications during or after procedure was recorded. Complications for fiducial placement was scored as per the Society of Interventional Radiology (SIR) grading system [13]. Pain score was done as per Wong-Baker pain scale [14]. Migration of fiducial after placement and during treatment were analyzed and presented in a separate manuscript. The present manuscript is focused on clinical parameters and scoring of fiducial placement.
2. Treatment planning and delivery
Contouring and treatment planning was done on Accuray MultiPlan version 5.3.0 (Accuray Inc., Sunnyvale, CA, USA). Treatment was started on day 4 post-fiducial placement and it was delivered through CyberKnife (M6 model, Accuray Inc.) [15,16]. Details of migration after placement and during treatment were analyzed. CT scan images were taken on day 0 (fiducial placement day), day 3 (CT simulation day) and at end of treatment (day 8). Analysis for fiducial migration was analyzed and will be presented in details in subsequent manuscript.
All the data was collected and analyzed with IBM SPSS version 22 (IBM, Armonk, NY, USA). Association between two categorical variables were assessed by cross tabulation and comparison of percentages. Chi-square test/Fisher exact test was used to test statistical significance. The p-value less than 0.05 was considered statistically significant.
Results
1. Demographic data
One hundred eight fiducials were placed in 36 patients—male, 92%, mean age, 60.2 years; Eastern Cooperative Oncology Group performance status (ECOG PS) 0–1, 92%; Child-Pugh A 89%, B&C 11%; majority in segments II and VI; PVT disease 64%—with HCCs (Table 3). Five patients (14%) had lesions in segment V, 8 patients (22%) had in segment VI, and 2 (6%) each in segments VII and VIII. Thirty-three patients (92%) had good performance status (PS 0–1). Only 3 patients (8%) had PS 2, but with small volume disease. Child-Pugh A, B, and C were 32 (89%), 3 (8%), and 1 (3%) patient, respectively. Twenty-nine patients (80%) were treated in five fractions, where as 16% and 4% in 3 and 4 fractions, respectively.

Fiducial placement related parameters (n = 108)
2. Fiducial placement related parameters
Fiducial placement under CT scan and ultrasound-guided were in 25 (69%) and 4 (19%) patients, respectively (Table 3). Time for placement was less than 20 minutes, between 21 and 45 minutes, and more than 45 minutes were in 20 (55%), 13 (36%), and 3 (8%) patients, respectively. All the patients had three fiducials placed under guidance. Post-fiducial severe pain score of 3–4 was only in 2 patients (6%). Majority of the patients had minimal pain (pain score 0–1, 26 patients, 72%) at 1-hour evaluation after placement. Recovery time after fiducial placement was usually less than 20 minutes in majority of the patients (29 patients, 80%). Only 5 patients (14%) had to be under supervision at day care and among them 1 patient (3%) required admission for hemothorax. Five patients (15%) had minor complications requiring intravenous medications (analgesics) (Fig. 1). Among the 5 patients who required admission in day care, 3 patients (9%) had pain abdomen and 2 patients (5%) had pneumothorax. One patient with pneumothorax recovered with supportive medication (oxygen), and 1 patient developed hemothorax and was transferred to intensive care. Three patients (8%) had major displacement (outside liver) immediately after the procedure: one in intestine (abdomen) and two in lung. Majority of the patients (92%) had no displacement after placement.

(A) Ideal placement of fiducial (X-ray anteroposterior topogram). (B) Fiducial migration to lung immediately after placement. (C, D) Fiducial migration to abdomen in computed tomography scan and X-ray anteroposterior topogram.
3. Evaluation of quality of fiducial placement
Among 108 fiducials placed, majority (24 patients, 67%) of the patients had fiducial placement score of 11–13 (good) (Table 4). Only 3 patients (8%) had poor (score 7) placement score, mostly due to post-fiducial sequel. Four patients (11%) had fair score (score 9–10) and 1 patient had very good score (score 14). Radiologist score of good was in 27 patients (75%), fair in 5 (14%) and poor in 2 (6%) patient, respectively. Radiation oncologist score was good in 26 (72%), fair in 7 (19%) and poor in 3 (8%) patients, respectively. Mean inter-fiducial distance range was 4.7 to 2.5 cm, inter-fiducial angle range was 82.7º to 28.5º, and distance from centre range was 2.1 to 5.1 cm, respectively. Concordance between radiologist score and radiation oncologist score was high (Table 5). Score of “poor” concordance was 2/2 (100%), “fair” score 4/5 (80%) and “good” score 24/27 (89%), respectively (p=0.001).

Evaluation the quality of fiducial placement (n = 108)

Concordance between radiologist score and radiation oncologist score (n = 36)
4. Factors influencing fiducial placement related parameters
Factors influencing fiducial placement related parameters are described in Table 6. Patients with poorer Child-Pugh score (p=0.080), poorer performance status (p=0.014) and patients accrued during the “learning curve” (p=0.013) had poor fiducial placement score. Recovery time was longer in patients with poor Child-Pugh score (p=0.025). Mean placement time was longer in patients with poor performance status (p=0.055). Major complications were higher in patients with poor performance status (p=0.009) and poor Child-Pugh score (p=0.034). Segment of liver involved (p=0.484) and the Barcelona Clinic Liver Cancer (BCLC) stage did not influence fiducial placement score.
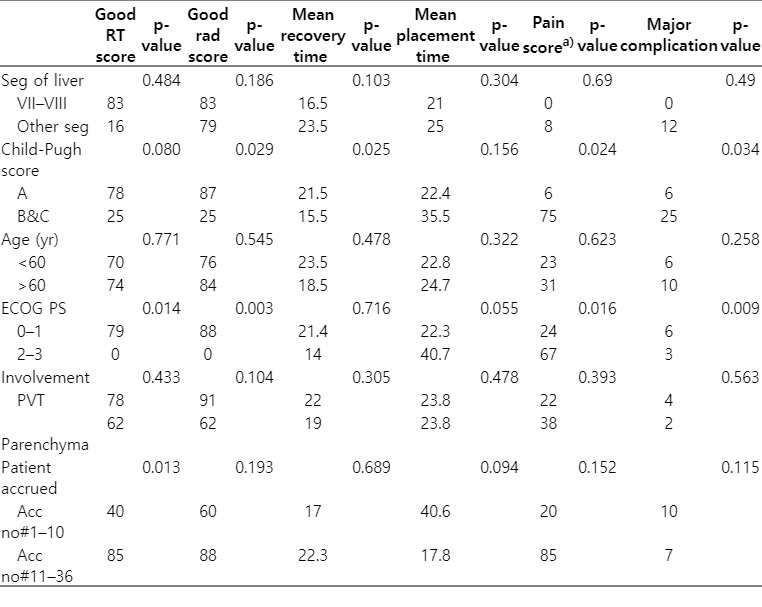
Factors influencing the fiducial related parameters
5. Learning curve for fiducial placement
There was significant difference in fiducial placement related parameters in first and last 10 patients accrued (Table 7). Good fiducial placement score was only in 30% in first cohort whereas 93% in last cohort (p=0.023). Time for fiducial placement was 42.2 and 14.3 minutes, respectively (p=0.069) in both the cohorts. Recovery time and complications also reduced with the learning curve. Learning curve in fiducial placement may also be due to accrual of relatively advanced patients during the early period of the study.
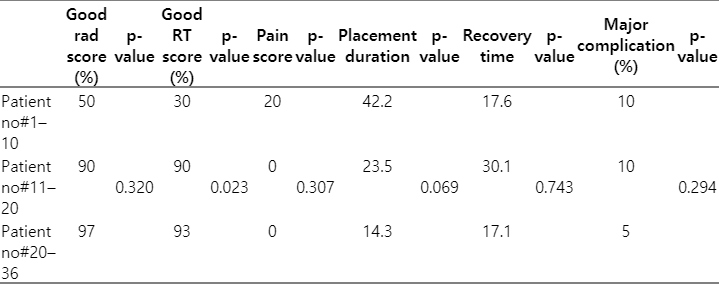
Patient and fiducial placement related parameters in different patient cohort
Discussion and Conclusion
Major bottle-neck for radiosurgery in liver tumour is fiducial placement [17]. There are apprehensions about “seeding” after implant as occurs in gallbladder cancer [8]. Complications such as pain, pneumothorax, migration, de-compensation of liver are major limitations of fiducial placement [5,6,18]. Complications are related to the patient condition and disease status [19,20]. More extensive diseases have higher probability of complications. Apprehensions about the procedure, patient counselling and support system also may influence the compliance and toxicity. Unfortunately, there are only a few published prospective studies evaluating the toxicity after fiducial placement, compliance and assessing the factors influencing the “quality” of fiducial placement [21,22]. The present prospective study has evaluated the quality of fiducial placement, factors influencing the quality of placement and also complications after placement. The present study also provides critical information regarding the complication rate in Indian patient population with extensive liver involvement and have relatively poor performance status.
In our study, the interventional radiologist termed 75% of placement as good with regards to accuracy compared to 72% by radiation oncologist. There was a good level of agreement between the radiation oncologist and interventional radiologist on the accuracy of fiducial placement. Segment of liver involved (segment VIII fiducial placement expected to have poorer fiducial placement score) did not show any significant difference. BCLC staging did not show any significant influence in fiducial placement. Patients with extensive liver involvement had poor fiducial placement score. Patient performance status and poorer Child-Pugh score patients had longer recovery time, longer fiducial placement time and higher probability of complications. Hence, the inclusion for fiducial placement and treatment is different. Patients with good performance status, less extensive disease with better Child-Pugh score are ideal candidate for fiducial placement with minimal complications. Better BCLC stage, better Child-Pugh score and small volume disease patients are ideal for radiosurgery treatment. Hence, patients with good performance status, preserved liver function, small volume disease and better Child-Pugh score are ideal candidate for radiosurgery treatment with fiducial placement. The proportion of people with successful fiducial placement in the liver was 92% in our study. Out of 3 patient (8%) who had gross fiducial displacement on the day of the procedure, two fiducials (5%) migrated into the lung and one fiducial (3%) migrated into the abdomen. There were no gross migrations seen during treatment or in immediate post treatment period. Post-fiducial placement 83% of patients had no complications. One patient (3%) had major complication in the form of liver decompensation resulting in death. Only 14% of patients had minor complications. Minor complications reported were pain, mild pneumothorax or fatigue post procedure requiring only symptomatic treatment. None of the patients had any complications during or post-treatment. The amount of pain reported post-fiducial placement was very minimal in the study, with the average pain score being 0.86. In literature, pain is the most common complication on any percutaneous procedure. Up to 84% of patients will have at least mild discomfort. When present, pain can usually be managed with short duration of analgesics or narcotics. Bleeding is the most important complication of liver puncture and can be severe when it occurs intraperitoneally [6,7]. Pneumothorax is a rare but serious complication after fiducial placement [5]. Tumour seeding risk is reported around 2.3% in biopsy group and 1% in radiofrequency ablation (RFA) group [8]. Fiducial migrations are uncommon but have implication in treatment delivery [23]. In our study, only 1 patient (3%) had severe adverse effect (death) due to hemothorax. Three patient (9%) had abdominal pain requiring intravenous medication and 2 patients had mild pneumothorax that was resolved with oxygen therapy. Only 5 patients (14%) required admission in day care for more than 1 hour, mostly for pain and pneumothorax management. The complication rates are similar to the published literature. The adverse effects were significantly higher in first ten patients, at the 'learning curve' period and had reduced after placement of adequate number of fiducials. This suggests, high volume centre with adequate exposure will have lesser complications. On the other hand, more advanced cases were accrued during the “learning phase”, and hence may have influenced higher morbidity during this period (case selection bias).
Park et al. [2] retrospectively reviewed 101 patients with ultrasound-guided intrahepatic fiducial placement. There were no major complications, although 12 patients (12%) developed minor complications. Technical success was achieved in 291 (97%) fiducial placement. Of 101 patients, 72 patients (71%) fiducials placement was ideal. Marsico et al. [5] assessed how different types of markers affects the tracking accuracy of CyberKnife. Ohta et al. [9] reported success rate of 100% (18/18) for fiducial placement in liver tumours. Only one patient (6%) had mild pneumothorax. There was no gross migration after placement. Oldrini et al. [21] evaluated the imaging technique for fiducial placement and concluded that ultrasound-guided placement is equivalent to CT guided placement. Rong et al. [24] evaluated the migration parameters after placement. Choi et al. [25] evaluated the safety and technical feasibility of endoscopic ultrasonography (EUS)-guided fiducial placement. Of 32 patients, 23 patients (91%) had successful placement and only 1 patient (3%) developed mild pancreatitis which subsided with supportive care. Kim et al. [3] evaluated the safety and technical success rate of an ultrasound-guided fiducial marker implantation. Twenty-one percent had minor complications. Abdominal pain was the most common complication (14%). Fiducial migration occurred in 5 patients (6.5%). Seppenwoolde et al. [22] in their study assessed the accuracy of day-to-day predictions of liver tumour position using implanted gold markers as surrogates and to compare the method with alternative set-up strategies (vertebrae and three-dimensional diaphragm-based set-up). Marker-guidance was superior to guiding treatment using other surrogates. Our study objectives were similar to that of Park et al. [2], Ohta et al. [9], and Choi et al. [25]. Mean age of our study population was 60 years and 92% were male. Similarly, Park et al. [2] reported mean age of 61 years and 73% were male in their study. Child-Pugh score was also similar in both the cohort (Child-Pugh A of 82% in our cohort and 89% in the study of Park et al. [2]). Liver segment involvement was also similar between the two cohort. In our study, all patients (n = 36) had three fiducials implanted. In the study of Park et al. [2], 97 (96%) out of 101 patients had three fiducials. Mean duration of fiducial placement was 23.8 minutes in our study. Time for fiducial placement, “quality” of placement and recovery time was not evaluated in any other study. In our study, mean maximum distance from the tumor center was 5.09, while minimum was 2.09 cm. Mean distance between marker and lesion in Park et al. [2] and Oldrini et al. [21] was 3.1 and 3.2 cm, respectively. Maximum and minimum mean inter-fiducial distance in our study was 4.77 and 2.54 cm, respectively. In the study of Oldrini et al. [21], mean distance between the markers was only 1.7 cm. Mean inter-fiducial angle was 82.7º (range, 12º to 117.5º) in our cohort. Successful fiducial placement was 33/36 (92%) in our cohort, whereas in the study of Park et al. [2], it was 97%. Migration immediately after placement was also similar in both the cohort (3% and 2.7%). In our cohort, no complications were seen in 83% and major complication in 1 patient (3%). Park et al. [2] also reported one (2.7%) had major complications and minor complication in 12%. In our cohort, two more patients (5.5%) had decompensation prior to start of treatment and hence treatment was withheld. Fourteen percent of patients had minor complications in the form of either pain, mild pneumothorax or fatigue post procedure which required symptomatic treatment only. Average pain score being 0.86 in our study. Pain scoring was not evaluated in the studies of Park et al. [2] and Choi et al. [25]. In our study, the interventional radiologist termed 75% of placement as good with regards to accuracy compared to 72% by radiation oncologist. There was a good level of agreement between the radiation oncologist and interventional radiologist on the accuracy of fiducial placement. The result in our prospective cohort was similar with the published literature from retrospective series.
The present study is unique in many ways. Strength of the study is that it is a prospective study with accrual of all consecutive liver patients had 108 fiducial placement and were treated with robotic radiosurgery. The self-devised fiducial placement scoring system, pain score and other parameters documented prospectively in all consecutive patients. The present study is one of the only few prospective studies evaluating the fiducial placement score and complications after fiducial placement in liver tumours. Major limitations of the study are relatively smaller sample size (108 fiducials). Scoring systems used for fiducial placement accuracy scoring, recovery grade, and fiducial migration were influenced by the Accuray fiducial system and SIR scoring system for complications, and may need an independent validation.
In summary, fiducial placement is safe and in experienced hands, “quality” of placement is “good” in majority. Major complications and admission after fiducial placement are rare. Complications, fiducial placement time, and recovery time are more during the “learning curve”. Patients with poor Child-Pugh score, extensive liver involvement, poor performance status have higher probability of complications. Segment of liver involvement and BCLC stage don’t influence fiducial placement “quality”. There is a case selection criteria for fiducial placement which is different from patient selection criteria for SBRT treatment.
Notes
Conflict of Interest
No potential conflict of interest relevant to this article was reported.
Acknowledgements
We acknowledge Department of Surgical Gastroenterology and Medical Oncology, Amrita Institute of Medical Science, Kochi for the support.