Introduction
Cutaneous squamous cell carcinomas (SCC) represent around 20%-30% of non-melanoma skin cancer [1]. The risk of developing non-melanoma skin cancer depends on genotypic, phenotypic, or environmental factors (residents of high ambient solar irradiance who have markers of ultraviolet susceptibility, fair skin, eye, and hair color, or an inability to tan, and skin disorders) [2]. The primary aim of treatment is the complete removal with good cosmetic result. Surgery is the most common and effective treatment [3], however it is necessary to maintain adequate margins (standard 4-5 mm). Some tumors are truly inoperable, due to the patient's inability to undergo removal or reconstruction, either because of the size or the anatomic location of the tumor. Furthermore some patients may nonetheless prefer a noninvasive treatment, such as radiation; in this instance brachytherapy (BT) is an excellent treatment option with a better result than external beam radiotherapy [4]. Curettage and electrodessication is recommended for SCC but not for large squamous-cell carcinomas and recurrent disease [2].
In these instances stereotactic body radiotherapy (SBRT) is an alternative to BT because it allows to deliver high doses of external radiation similar to BT dose distribution [5] using multimodal imaging [6]. Modern external beams radiation therapy, such as stereotactic technique that is able to deliver high doses in targeted complex shapes. CyberKnife (Accuray Inc., Sunnyvale, CA, USA) is a robotic device used to treat both intracranial and extracranial targets. The aim of this study is to report on the CyberKnife technique, dosimetry and acute skin toxicity after treatment in a patient with SCC of the nasal bridge, as alternative technique to BT. Using radiation therapy a common side effect is the occurrence of skin toxicity varying from erythema to ulcer; in these circumstances the treatment of choice is topical use of corticosteroid and in cases of superinfection antibiotics. We report on an elderly patient treated for SCC using stereotactic technique.
Case Report
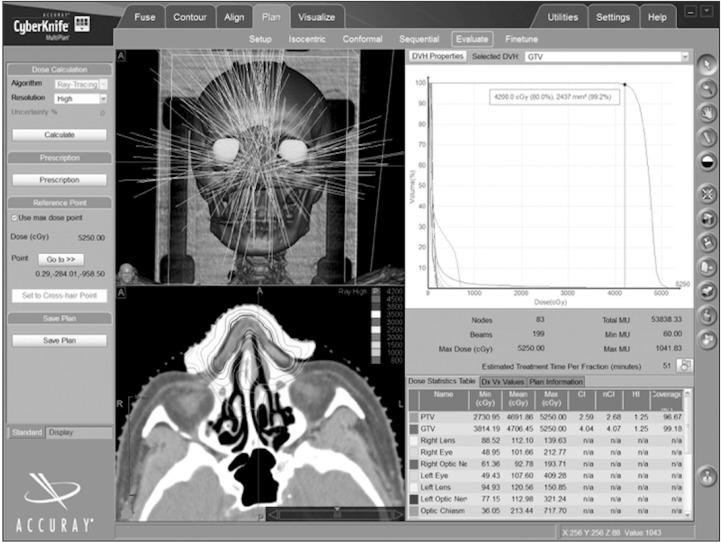
An 82-year-old Caucasian female had a three years history of cutaneous lesion on the nose which increased in extension in the last three months occupying the entire nasal bridge (3 cm × 4 cm). A biopsy confirmed a well-differentiated SCC and a computed tomography (CT) demonstrated the absence of invasion of bone and cartilaginous tissue without neck node involvement (February 2013). The presence of comorbidities and the dimension of the SCC contraindicated a surgical approach. For this reason the patient was referred to our department. We choose to treat this case using stereotactic technique with CyberKnife, a robotic linear accelerator based stereotactic device. For the SBRT set-up the patient was placed supine on the treatment couch and immobilized with a custom-fitted thermoplastic mask (Orfit Industries America, Jericho, NY, USA) and a bolus was used on skin surface (Fig. 1). The CT (Siemens SOMATOM Sensation 16; Siemens AG Medical Solutions, Erlangen, Germany) protocol followed specific requirements for the CyberKnife system: acquisition 16 × 0.75 mm, 120 kV, 320 effective mAs, pitch 1.15; and reconstruction slice 1.5 mm, reconstruction increment 1.5 mm, filter reconstruction H31 (smooth), 512 × 512 matrix. The MRI (Siemens MAGNETOM 1.5-T) protocol was performed with the following parameters: matrix 512 × 512, flip angle 0°, effective thickness 0.88 mm, reconstruction slice 1.5 mm, reconstruction increment 0 mm. The axial source images were transferred to the CyberKnife workstation for treatment planning (MultiPlan treatment planning system, Accuray Inc.) for SBRT modality. The contouring of the tumor and critical organs were defined with CT imaging. For SBRT, the clinical tumor volume (CTV) was obtained by the gross tumor volume plus an isotropic expansion of 4 mm in all directions except anteriorly and posteriorly; the planning target volume corresponded to CTV. The SBRT treatment planning was obtained with inverse planning algorithm using a nonisocentric technique. A heterogeneous dose distribution was generated to emulate high-dose rate brachytherapy [7] (Fig. 1).
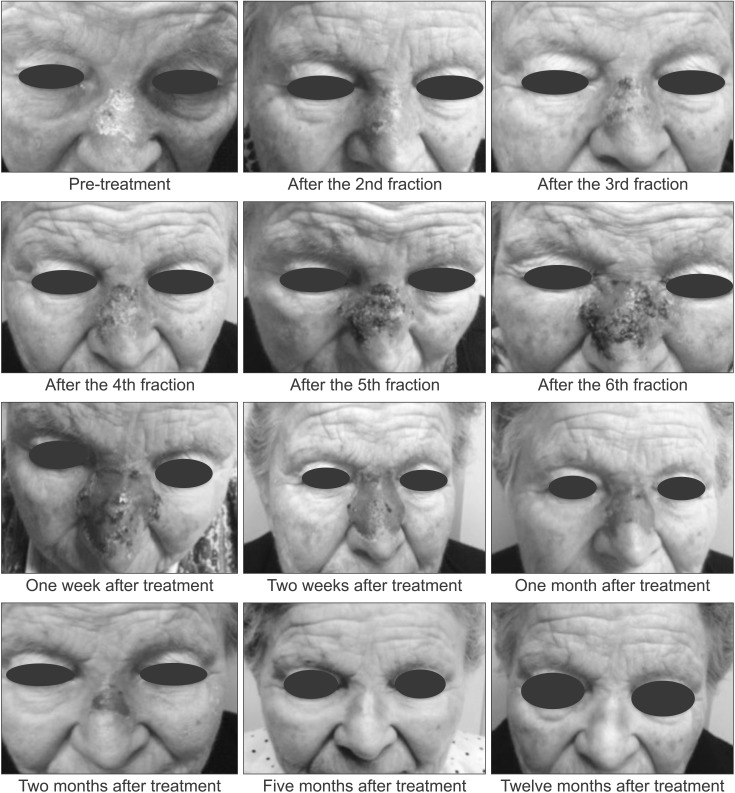
We utilized fixed collimator with different diameter: 7.5, 10.0, and 12.5 mm. The volume of the tumor was 2.5 mL. The dose [8] to the target was 4,200 cGy delivered in 6 sessions in 3 weeks (2 fractions for week) prescribed to the 80% isodose line. The maximal dose (Dmax) was 5,250 cGy. The coverage of the target was 96.7%, the number of beams was 199, the conformality index 2.59, the homogeneity index 1.25, and the new conformality index 2.68. The number of total monitor unit was 53,838. The Dmax at the critical organs for all six fractions was 193.71 cGy at right optic nerve, 212.28 cGy at right eye, 139.63 cGy at right lens, 321.24 cGy at left optic nerve, 409.28 cGy left eye, 150.85 cGy left lens, and 717.70 cGy at optic chiasm. The acute toxicity was evaluated during irradiation; the peak toxicity was measured after 1 week post-treatment. Toxicities were recorded using Common Terminology Criteria for Adverse Events (CTCAE) ver. 3. The patient after the fifth fraction, in the third week of treatment, showed an acute reaction (Fig. 2) characterized by desquamation, dermatitis, and ulceration (G3). For this reason we commenced with topical therapy using Vea Sil (Hulka srl, Rovigo, Italy) a thin sterile silicone (lamina) and vitamin E (using topical alpha-tocopherol acetate [α-TA]). The lamina can be applied in difficult areas (nasal root, elbow, knee, etc.). This treatment started in the last week of SBRT therapy and carried on six weeks after irradiation (Fig. 2).
The patient was examined 12 months after treatment. A complete clinical remission with excellent cosmetic and functional result without disease recurrence was obtained (Fig. 2). No recurrences were observed 24 months after treatment. The patient gave consent for the case reports to be published.
Discussion
The best cosmetic and functional result can be obtained with radiotherapy in cases of SCC of the lip, nose, and ear [3]. Additionally, long-term results of SCC treated with radiotherapy are similar to those of other treatment modalities [9101112]. Using SBRT we obtained a long-term and complete clinical remission, preserving anatomical functionality. The primary benefit of SBRT is similar to BT and it is able to deliver radiation to the target tissue with less injury to the surrounding normal-appearing skin. The rapid drop-off of SBRT, in inverse planning modality, permits to deliver a homogeneous dose distribution. The conformality and target coverage was obtained even in difficult anatomical areas.
We believe that our therapeutic approach is feasible and could be proposed for elderly patients who refuse BT, or frail patients not suitable for a surgical approach. In fact, in daily clinical practice many patients have 'irregular and difficult' SCC and it is important that radiation oncologists have more therapeutic options in these instances [13]. The use of electrons or orthovoltage X-ray in SCC is conditioned from irregularity of some anatomical areas. Besides there are limits linked to the use of collimators and the daily setup position. The SBRT with image guided exceeds the limits of the set-up for relocation; the inverse planning allows covering irregular volumes and the use of the photons 6-MV X-rays permits to treat inner lesions.
We underline that this is the first case report on this issue using SBRT. Considering the actual worldwide availability of stereotactic devices, it is important to report this case so more patients might utilize a conservative approach with both esthetic and functional preservation.
Skin care for radiation therapy patients can be a controversial subject for the different practices among institutions and individual practitioners. The most common side effects reported, after BT, include crust formation, dryness, and adhesions. Less frequent are soft tissue necrosis and chronic pain. Late side effects like chondronecrosis occur in 10% to 15% of patients, however, the relationship between total dose and/or fractionation regimen and toxicity is unclear [14]. None of these late side effects to date was reported by our patient.
A Canadian survey [3] found considerable differences among institutions in the prevention and management of acute radiation skin reactions. Inconsistencies among practitioners can lead to patients receiving conflicting or even erroneous information.
In radiation therapy centers dry desquamation or moist desquamations are often seen. The objective when managing dry desquamation is to alleviate discomfort. Skin hydration has been recommended to relieve symptoms of dry skin and to reduce further aggravation associated with pruritus that leads to secondary infection and pain, which could worsen the quality of life [15]. In moist desquamation the skin becomes open and susceptible to infection, and antibacterial or antifungal medications are currently prescribed. However, when there is no proven infection, the routine use of antiseptics, antibiotics, and disinfectants is questionable [15]. The opposite is true for moist desquamation, in that the skin breaks down and becomes susceptible to infection, for which antibacterial or antifungal medication is currently prescribed [16]. Stanizzi et al. [17], using topical α-TA in 35 patients with exudates, pain and delayed re-epithelialization in absence of tissue necrosis and/or sepsis, reported a quicker reduction of exudates and pain and faster wound healing in all patients. α-TA seems to reduce bacterial growth and improves epithelialization. In our case the use of a lamina of silicone containing vitamin E (Vea Sil) allowed to cure the moist desquamation in the absence of bacterial and fungal infections. Our experience demonstrates the efficacy of SBRT in the treatment the SCC of the face, even if more data are necessary to confirm our observation.