Atlas of sentinel lymph nodes in early breast cancer using single-photon emission computed tomography: implication for lymphatic contouring
Article information

Abstract
Purpose
To determine the localization of sentinel lymph nodes (SLNs) in a large cohort of patients with breast cancer and validate the European Society for Therapeutic Radiology and Oncology (ESTRO), Radiation Therapy Oncology Group (RTOG), and Radiotherapy Comparative Effectiveness (RADCOMP) guidelines on regional lymph node clinical target volume (CTV-LN) delineation.
Materials and Methods
A total of 254 women with cT1-3N0-1M0 breast cancer underwent single-photon emission computed tomography (SPECT-CT) visualization of SLNs after intra- and peritumoral injection of 99mTc-radiocolloids. All SPECT-CT images were fused with reference simulation computed tomography. A 3D atlas of SLNs was created and used for evaluation of CTV-LN defined by contouring guidelines.
Results
SPECT-CT visualized 532 SLNs that were localized in axillary level I in 67.5%, level II in 15.4%, level III in 7.3%, internal mammary in 8.5%, and supraclavicular in 1.3% cases. The majority of level II–IV and internal mammary SLNs were inside the recommended CTV-LN. Axillary level I SLNs were covered by ESTRO and RTOG contours in 85% and 85% cases, respectively. “Out of contours” SLNs were mostly detected in lateral subgroup of level I LN (18.5%), while 98%–99% of anterior pectoral and central axillary SLNs were covered by CTV-LN. Internal mammary SLNs were visualized in 33 cases and were outside ESTRO and RTOG contours in 3 and 6 observations, respectively.
Conclusion
SPECT-CT atlas of SLNs demonstrated that in most cases ESTRO and RTOG guidelines correctly represented CTV-LNs with the exception of lateral subgroup of SLNs.
Introduction
The concept of sentinel lymph nodes (SLNs) was proposed in the last quarter of the 20th century and was extensively evaluated in patients with melanoma and breast cancer [1]. The concept postulated a predictive and sequential fashion of regional lymph node (LN) involvement with the regional spread predominantly to the LNs that were the first on the drainage way from the primary lesion (these LNs were called sentinel); subsequent invasion of the second echelon LNs that received lymph fluid from the sentinel nodes; and finally with a regional dissemination of the tumour to other regional LNs. This concept was successfully validated in prospective multicentre trials and retrospective meta-analysis and now is widely accepted in clinical practice [1–3]. Mapping of SLNs by radiocolloids becomes the basic technique that permits a precise localization of SLNs and a subsequent radioguided surgery. Taking into account the sequential order of regional LNs involvement and prevalence of SLNs invasion by the tumour, we propose that the atlas of SLNs can be an effective tool that would help to validate the most widely used European Society for Therapeutic Radiology and Oncology (ESTRO) and Radiation Therapy Oncology Group (RTOG) guidelines for contouring regional LNs in patients with breast cancer. We expect that this atlas can be especially useful as a tool for a precise definition of LN clinical target volume (LN-CTV) in women with an early breast cancer. First of all, it can be important for LN contouring in women with N1 breast cancer and patients with positive SLNs that would receive postoperative LNs irradiation instead of an axillary LNs dissection.
The primary aim of the this study was to create a 3D atlas of SLNs in patients with early breast cancer using single-photon emission computed tomography (SPECT-CT) and evaluate the validity of ESTRO, RTOG, and RADCOMP (Radiotherapy Comparative Effectiveness) Consortium Trial contouring guidelines [4–6].
Materials and Methods
This study was reviewed by review board and Ethical Committee of the N.N. Petrov National Medical Research Center of Oncology (No. 108). A total 254 women with an early (T1-3N0M0) breast cancer underwent SPECT-CT visualization of SLNs before a routine SLN biopsy between February 2014 and April 2020. The SPECT-CT examination started 60-120 minutes after intra- and peritumoral injection of 100–150 MBq of 99mTc-radiocolloids with particle size of 80–1,000 nm. The acquisition was performed in position with arms 140°–170° abducted above the head. The anatomical position of SLNs on SPECT-CT images was allocated to the following axillary subgroups that had been previously described in details [7]: anterior pectoral, central and lateral level I LNs, subscapular, interpectoral, subpectoral level II LNs, apical level III LNs. In addition, supraclavicular and internal mammary LNs were considered as regional for breast cancer patients. All SLNs were contoured on every SPECT-CT data set and color-coded according to their allocation to different groups and subgroups of the regional LNs. Finally we obtained images of 135 women with left (289 SLNs) and 243 (243 SLNs) with right breast cancer.
For the reference CT image we used a simulation CT scan of a female patient (164 cm, 60 kg) who had undergone a left-sided breast conserving surgery and irradiation per standard protocol.
It was reported by Dijkema et al. [8] that localization of the regional LNs of the breast can be dependent on the position of the arm. In order to compare LN coverage by planning contours in different treatment positions, we performed CT simulation of the reference patient in treatment position with 130° abducted left arm and 160° overhead abducted right arm.
Atlas creation and statistical analysis of the SLN overlap data was performed using MIM Maestro 6.9.7 software (MIM Software Inc., Cleveland, OH, USA). The atlas was created using the approach similar to the one described by Borm et al. [9]. First, the images were masked outside of the regions of interest corresponding to a 5-cm margin around to reference areas. Initial rigid registration of the masked images was followed by a contour-based deformable registration using a hybrid fusion mode [10] provided by MIM Maestro software. MIM Maestro Reg Refine tool was used to assess the quality of deformable registration and to enable user-guided deformable registration adjustment as necessary [11]. Next, each SLN contour on the patient image was deformable transferred to the reference patient CT image. All steps were automated using MIM Maestro Workflows to standardize and speed up image processing for each patient. Following the atlas creation, a statistical overlap (occurrence of the SLN contours inside CTVs) was calculated using a custom MIM Maestro Extension written in Java programming language, with the overlap statistical data being exported into Excel Software (Microsoft, Redmond, WA, USA) for subsequent verification and analysis. The CTVs for LN irradiation were delineated by two experienced radiation oncologists with a cross-evaluation of the contours and a subsequent control by the third investigator. All contours were delineated according to ESTRO or RTPOG guidelines [4,5]. All CTVs were created before the fusion by radiation oncologists that were blinded to the locations of SLNs. The contoured subregions corresponding to ESTRO and RTOG guidelines were as follows: axillary level I, II, and III LNs, the supraclavicular, the internal mammary, interpectoral and subpectoral region. In addition, we created a separate “posterior neck volume” which was represented by the differences in RADCOMP and ESTRO/RTOG volumes.
Finally, we calculated the overlap of mapped SLNs with “standard” LNs CTV contours and assessed whether they were located within/partly within (10%–100% overlap) or outside (<10% overlap) the ESTRO/RTOG and RADCOMP CTVs.
Results
In 254 women included in the study, we visualized 532 SLNs in average 2.1 SLNs per patient. Atlas of the mapped SLNs in relation to the ESTRO and RTOG CTV-LN can be found in Supplementary Figs. S1 and S2. The distribution of SLNs according to LN levels is summarized in Table 1. As was expected, most SLNs were detected in the axillary level I region (n = 359; 67.5%), followed by axillary II (n = 82; 15.5%), axillary III (n = 39; 7.3%), the internal mammary (n = 45; 8.4%), and supraclavicular (n = 7; 1.3%) regions. Mapped LNs in apical (level III) and supraclavicular regions probably must be considered as second echelon LNs that are directly connected with axillary SLNs. This proposal is supported by the fact that in all cases axillary SLNs were detected before “hot” LNs of apical and supraclavicular regions. Distribution of the LNs that were mapped with radiocolloids according to axillary (level I) subgroups is listed in Table 2. SLNs were located in the central axillary subgroup in 171, anterior pectoral in 135, lateral in 49, and subscapular in 4 cases. The distribution of mapped LNs in patients did not differ between right and left breast cancer.
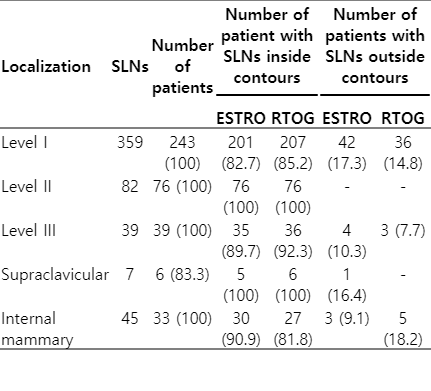
Distribution of SLNs in the lymph node regions and coverage of these lymph nodes by ESTRO and RTOG contours
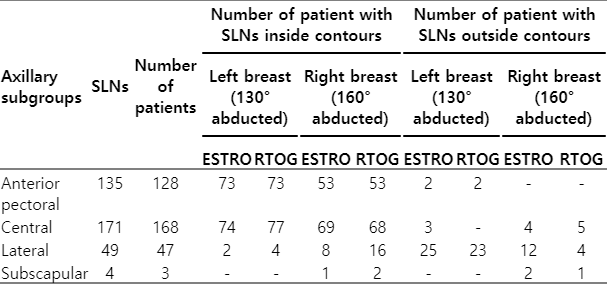
Distribution of SLNs in the axillary lymph node subgroups and coverage of these lymph nodes by ESTRO and RTOG contours in women with different arm positions
1. Level I lymph nodes
SLNs detected in the axillary level I were outside the ESTRO guideline borders in 42 of 243 patients with mapped level I LNs and outside RTOG LNs CTV in 36 of 243 cases. Surprisingly, we found that SLNs were frequently localized in the lateral group of axillary LNs (Fig. 1): in 47 (19.3%) women SLNs were revealed in the lateral group, and in 14 cases SLNs were detected only in the lateral group. It must be pointed out that in many cases SLNs of the lateral group were localized out of the ESTRO and RTOG contours: 37/47 and 27/47 observations, respectively. This is due to the position of the arm that significantly influences the rate of “in contours” and “out of contours” localization of the lateral group SLNs. In 119 women with the right breast cancer (160° abduction), 12 of 20 SLNs in the lateral group were inside ESTRO and 16 of 20 inside RTOG contours. With 130° abduction (left breast), lateral group SLNs were visualized “out of ESTRO contours” in 25 of 27 cases and out of RTOG borders in 12 of 27 patients.

Lateral subgroup of axillary lymph nodes (blue) that are mostly out and partly inside the RTOG and the ESTRO contours. (A) Axial image represent lateral (blue), central (red), and anterior pectoral (green) subgroups of axillary lymph nodes in relation to ESTRO contours (green) and RTOG contours (yellow). (B) Coronal image of left lateral axillary lymph nodes. (C) Coronal image of right lateral axillary lymph nodes. ESRTO, European Society for Radiation Therapy and Oncology; RTOG, Radiation Therapy Oncology Group.
As it was mentioned above, in most cases level I axillary SLNs are represented by anterior pectoral and the central LNs. These SLNs are usually successfully covered by LNs CTV recommended by ESTRO (n = 299 of 306 visualized SLNs, 97.7%) and by RTOG (n = 302 of 306 visualized SLNs, 98.7%). SLNs of central subgroup were not covered by ESTRO CTV in seven women: 1 mm anterior and 1 mm, 5 mm, 9 mm, 9 mm, 11 mm, 11 mm caudally from the ESTRO border. Central SLNs were out of RTOG contours in five cases: 1 mm, 4 mm, 4 mm, 9 mm, and 10 mm caudally from the RTOG border. Anterior pectorals SLNs were 1 mm and 2 mm anterior-laterally from ESTRO CTV contour in two women and 2 mm anterior to RTOG CTV in one observation. We did not find any correlation between the position of the arm and the number of “out of contours” anterior pectoral and central LNs.
In the case of tangential irradiation, this “anterior shift” of the LNs CTV can potentially reduce the absorbed doses in the heart, coronary vessels (left breast), and lung but this proposal of course needs further evaluation.
We compared the coverage of the SLNs by ESTRO and RTOG contours in patients with a different arm position (left breast vs. right breast). The only and important finding was much better coverage of SLNs localized in the group of lateral axillary LNs: with 160° abducted arm (right breast), they were covered by ESTRO and RTOG contours in 8 (40%) of 20 and 16 (80%) of 20, respectively. On the contrary, in patients with 130° abduction (left breast), SLNs localized in the lateral axillary group were inside of RTOG and ESTRO volumes only in 2 (7.4%) of 27 and 4 (14.8%) of 27 cases.
2. Level II and III lymph nodes
SLNs were localized on axillary level II in 71 patients, and in all cases they were successfully covered by ESTRO and RTOG contours. Subpectoral SLNs were usually localized very close (Supplementary Fig. S3) to the thoracic vault (48 observations). This fact underlines the necessity to cover the anterior surface of the I–III ribs carefully.
“Hot” LNs with uptake of radiocolloids on axillary level III and supraclavicular LNs were visualized in 39 and 7 patients. In all cases, radioactive LNs in these regions were accompanied by SLNs in level I and/or II. Apical “hot” LNs were outside the ESTRO and RTOG contours in four and three women: 1 mm, 1 mm, 8 mm, 9 mm cranially and 3 mm, 3 mm, 4 mm cranially, respectively.
3. Supraclavicular lymph nodes
The topography of SLNs in supraclavicular region can be important for better understanding the minimal and sufficient borders of supraclavicular CTV. First of all, we evaluated the guidelines of RADCOMP trial that recommend irradiation of posterior neck region. According to our data there were no SLNs in posterior neck in any of our six patients. Secondly, we tried to evaluate the most medial location of SLNs in supraclavicular region and found out that there was only one SLN medial to vein and we did not see any SLN medially to the common carotid artery (Fig. 2). Only one “out of ESTRO contours” SLN was visualized 1 mm caudally to the upper border of the supraclavicular contours but was inside RTOG contours.

Localization of the supraclavicular lymph nodes (blue) with uptake of radiocolloids with regard to the European Society for Radiation Therapy and Oncology contours (green) and the Radiation Therapy Oncology Group contours (yellow).
4. Internal mammary lymph nodes
SLNs in the internal mammary region were revealed in 33 (13%) of 254 evaluated patients: eight on the right side and 25 on the left. In all cases they were detected between the I rib and the IV rib. Only three internal mammary SLNs were out of ESTRO contour: 1 mm anterior, 1 mm and 2 mm laterally from CTV border. Internal mammary LNs were out of RTOG contour in six cases: 1 mm, 1 mm, 2 mm anterior-medially, 2 mm anterior-laterally, and 1 mm, 2 mm laterally. Obtained data indicate that 7 mm margins around internal mammary vessels would help to cover internal mammary SLNs in all cases.
Discussion and Conclusion
For our knowledge this is the first attempt to evaluate different international guidelines for regional LN delineation by mapping SLNs topography in large population of patients with breast cancer. A detailed SLN atlas was created using SPECT-CT data of 254 women with an early breast cancer and a non-rigid registration of these data based on vessels and muscles anatomy. An important finding of this study is the variability of lymphatic drainage from breast lesions that manifested by various localization of radioactive LNs represented by sentinel LNs and second echelon LNs which were the next step of the regional metastatic pathway. According to our data 82.9% of SLNs were visualized in axillary level I and II. This is in accordance with existing PET-CT data indicating that the majority of metastatic lymph nodes in primary patients with breast cancer are located in the axilla (91.6%) [9]. According to Kowalski et al. [12] in patients with advanced and recurrent disease regional metastases detected in the axillary LNs in 73% of all cases and in other 27% occupied internal mammary and supraclavicular regions.
Our results surprisingly demonstrated that only 82%–85% of level I LNs were covered by contours created according to ESTRO and RTOG guidelines. In most cases, “out of contour” LNs represented by SLNs were localized in the lateral axillary subgroup (37/42 in ESTRO and 27/36 in RTOG). Generally, these LNs are not considered as regional LNs receiving the lymph flow from the breast but represent the nodes that collect lymph flow from the arm and hence, are not the target for regional LN irradiation [13]. It must be pointed out that in studies that evaluate the pattern of regional recurrences in patient with breast cancer these nodes are rarely pointed out as “the risk area.” On the other hand, the low frequency of regional recurrences in lateral axillary LNs can be explained by the high therapeutic dose that they absorb during the tangential irradiation of the breast [7]. The tendency to more complex and accurate methods of the dose delivery to the breast and LNs CTV (proton therapy, intensity-modulated radiotherapy) can be associated with a substantial underdose of lateral axillary LNs and a subsequent increased frequency of regional recurrences in this area [14]. It seems that in these cases lateral lymph nodes must be included in the LN-CTV. According to our personal experience, the irradiation in the position of 160° overhead abducted right arm with 1–2 cm lateral expansion of level I LN-CTV can help to cover lateral axillary LNs in most cases.
In addition, we mentioned one regularity that could be important for radiotherapy planning: if in women with 130° abducted arm (left breast) we would draw imaginary lines connecting the anterior-lateral surface of the II–V ribs with anterior surface of latissimus dorsi muscle (Fig. 3) all central, anterior-pectoral and lateral SLNs would be localized anterior to this line. The same pattern was detected in patients with 160° overhead abducted arm with the imaginary line passing nearly horizontally.

Axial images of the left axillary lymph nodes. Yellow line represents the plan that connects the anterior-lateral surface of the II–V ribs and anterior surface of latissimus dorsi muscle. All anterior pectoral (green) and central (red) axillary lymph nodes are visualized anterior to this plan. (A) On the level of the II rib. (B) On the level of the III rib. (C) On the level the V rib.
It is well-known that in women with breast cancer radiotherapy significantly increases the risk of late complications. First of all, morbidity and mortally associated with cardiac disease, in particular it was demonstrated that cardiac mortality was strongly related to the dose absorbed by the heart [15,16]. Additionally, it was shown that radiotherapy could increase the incidence of primary lung, esophageal and contralateral breast cancers [17–19]. Our mapping results indicate that localization of SLNs on the axillary level I give the opportunity to move forward the posterior border of the level I contours and significantly reduce the irradiated volume and doses absorbed by heart (in left-sided breast cancer), lung and contralateral breast.
Existing studies that conducted a three-dimensional analysis of LN recurrences and/or topography of LN metastases in patients with breast cancer indicate that around 13%–34% of regional recurrences were located in the supraclavicular LNs [9,19,20]. According to the study by Chang et al. [20], supraclavicular LNs were the most frequent site of regional recurrences (33.8%); DeSelm et al. [19] revealed supraclavicular LNs metastases in 25.5%; and Borm et al. [9] in 13.8%. According to our data, only 2.3% of evaluated patients had radioactive (“hot”) LNs in supraclavicular area and as was mentioned before we believe that most of these LNs were second echelon nodes. We found out that all these LNs were located laterally to common carotid artery and caudal to cricoid cartilage. Nielsen and Offersen [21] also concluded that ESTRO contours of supraclavicular area were correct and did not need enlargement. On the contrary, many authors reported that mapping of supraclavicular recurrent or clinically involved LNs demonstrated that around 20%–41% of metastases in this region were located out of RTOG and/or ESTRO contours and nearly always associated with an advanced nodal disease [9,12,20,22]. Usually missed metastatic supraclavicular LNs were found laterally to sternocleidomastoid muscles, posterior to the transverse process of the vertebral body [19,22,23] or cranial to the subclavian artery [24] mostly at the level of thyroid and cricoid cartilage [25]. Gee et al. [14] summarizing the existing studies mentioned that the most vulnerable to geographical miss were the cranial and posterolateral contours of supraclavicular area.
Prospective randomised and observation studies, retrospective analysis of these trials showed that irradiation of internal mammary LNs could improve overall and distant metastatic free survival [26-28]. We visualized SLNs in internal mammary region in 33 (13%) of 254 evaluated patients. All these SLNs were located cranially to the 4th rib and were successfully covered by ESTRO and RTOG contours. These data is in accordance with the previous experience that indicated that 90% of metastatic internal mammary LNs were detected in the 1st–3rd intercostals spaces [12,24,29] and were successfully covered by ESTRO, RTOG, and RADCOMP contours.
Our data have several important limitations. In contrast with previous studies that mapped recurrent or FDG-positive LNs we evaluate topography of sentinel and second echelon LNs—nodes with the highest risk of involvement in patients with an early breast cancer. This means that our data must be used with caution in women with the advanced nodal disease and can be more applicable for women with 1–3 positive LNs or in case of irradiation after positive sentinel LN biopsy. It must be also mentioned that all women who underwent SPECT-CT examinations had an early breast cancer (T1-3N0-1M0).
Moreover, despite the deformable algorithm of fusion the accuracy of this procedure can be slightly compromised by a difference in arm position between SPECT-CT and simulation CT.
In conclusion, SPECT-CT atlas of SLNs demonstrated that in most cases ESTRO and RTOG guidelines were effective for contouring of axillary II–III, supraclavicular and internal mammary LNs. In 18.5% of evaluated patients, SLNs were located in lateral axillary subgroup that in most cases was not covered by ESTRO and RTOG contours. These data must be specially considered in cases when tangential irradiation is substituted by intensity-modulated radiotherapy or proton therapy. Our data indicate that in patients with 1–3 positive LNs posterior border of level I axillary LNs can be safely shifted anteriorly (to the imaginary line connecting anterior-lateral surface of the II–V ribs with anterior surface of latissimus dorsi muscle) that would help to reduce absorbed doses in lung and heart.
Notes
Conflict of Interest
No potential conflict of interest was reported by the authors.
Acknowledgements
The authors would like to acknowledge MIM Software Inc. (Cleveland, OH, USA) for providing MIM Maestro software used in this study and Dr. Oleg Egorov for enabling the automation of image processing and statistical analysis.
Supplementary Materials
Supplementary materials can be found via https://doi.org/10.3857/roj.2020.00871.
Atlas of sentinel lymph nodes represented on computed tomography simulation of the reference patient with regard to the European Society for Therapeutic Radiology and Oncology (ESTRO) consensus guideline on lymph node delineation. Clinical target volume contours: level I (yellow), level II subpectoral (green), level II interpectoral (orange), level III (red), supraclavicular (blue), and internal mammary (pink). Lymph nodes subgroups: central (red), central thoracic wall (purple), anterior pectoral (green), lateral (blue), subscapular (dark green), subpectoral (pink), interpectoral (light green), apical (orange and yellow), and internal mammary (magenta). Central and anterior pectoral level I lymph nodes are nearly always covered by ESTRO contours. On the contrary, lateral lymph nodes in most cases are out of ESTRO contours. In the position of 160° overhead abducted right arm some level I lymph nodes (central group) can be localized below the caudal contour. Nearly all level II, level III lymph nodes are successfully covered by ESTRO contours. We found out that all supraclavicular nodes were located laterally to the common carotid artery and caudal to cricoid cartilage (inside ESTRO contour). Internal mammary lymph nodes are localized outside the Radiation Therapy Oncology Group (RTOG) contour in 5 of 33 cases (18%) and can be covered by 7 mm additional margins.
Atlas of sentinel lymph nodes represented on computed tomography simulation of the reference patient with regard to the Radiation Therapy Oncology Group (RTOG) and Radiotherapy Comparative Effectiveness Consortium Trial (RADCOMP) atlases for radiation therapy planning. Clinical target volume contours: level I (yellow), level II (green), level III (blue), supraclavicular (pink), internal mammary (red), and RADCOMP posterior neck volume (dark blue). Lymph nodes subgroups: central (red), central thoracic wall (purple), anterior pectoral (green), lateral (blue), subscapular (dark green), subpectoral (pink), interpectoral (light green) apical (orange and yellow), and internal mammary (magenta). Central and anterior pectoral level I lymph nodes are nearly always covered by RTOG contours. In women with 130° abducted left arm most lateral lymph nodes are out of RTOG contours but in the position of 160° overhead abducted right arm 80% of lateral lymph nodes are on the border or inside RTOG contours.
Localization of the subpectoral lymph nodes with uptake of radiocolloids with regard to the European Society for Therapeutic Radiology and Oncology (ESTRO) and Radiation Therapy Oncology Group (RTOG) contours. All subpectoral lymph nodes are covered by both ESTRO and RTOG contours. Very close location of subpectoral nodes to thoracic vault demonstrates the necessity to cover anterior surface of the I–III ribs. RTOG contours (yellow), ESTRO contours (green), subpectoral lymph nodes (brown), anterior pectoral (green), central (red), lateral (blue), and interpectoral (light green).