Effect of early chemoradiotherapy in patients with limited stage small cell lung cancer
Article information
Abstract
Purpose
We evaluated the effect of early chemoradiotherapy on the treatment of patients with limited stage small cell lung cancer (LS-SCLC).
Materials and Methods
Between January 2006 and December 2011, thirty-one patients with histologically proven LS-SCLC who were treated with two cycles of chemotherapy followed by concurrent chemoradiotherapy and consolidation chemotherapy were retrospectively analyzed. The chemotherapy regimen was composed of etoposide and cisplatin. Thoracic radiotherapy consisted of 50 to 60 Gy (median, 54 Gy) given in 5 to 6.5 weeks.
Results
The follow-up period ranged from 5 to 53 months (median, 22 months). After chemoradiotherapy, 35.5% of the patients (11 patients) showed complete response, 61.3% (19 patients) showed partial response, 3.2% (one patient) showed progressive disease, resulting in an overall response rate of 96.8% (30 patients). The 1-, 2-, and 3-year overall survival (OS) rates were 66.5%, 41.0%, and 28.1%, respectively, with a median OS of 21.3 months. The 1-, 2-, and 3-year progression free survival (PFS) rates were 49.8%, 22.8%, and 13.7%, respectively, with median PFS of 12 months. The patterns of failure were: locoregional recurrences in 29.0% (nine patients), distant metastasis in 9.7% (three patients), and both locoregional and distant metastasis in 9.7% (three patients). Grade 3 or 4 toxicities of leukopenia, anemia, and thrombocytopenia were observed in 32.2%, 29.0%, and 25.8%, respectively. Grade 3 radiation esophagitis and radiation pneumonitis were shown in 12.9% and 6.4%, respectively.
Conclusion
We conclude that early chemoradiotherapy for LS-SCLC provides feasible and acceptable local control and safety.
Introduction
Small cell lung cancer (SCLC) accounts for about 15% of lung cancers and approximately 30% to 40% of these patients are limited stage (LS) SCLC [1].
A combination of chemotherapy and thoracic radiotherapy (TRT) is preferable to chemotherapy alone in the management of LS-SCLC [2,3]. Two meta-analysis studies have shown that combined chemotherapy with TRT in LS-SCLC significantly reduces local recurrence and improves overall survival (OS) [4,5]. In addition, the following meta-analysis and phase-III clinical trials reported that a concurrent chemoradiotherapy (CCRT) regimen was superior to a sequential one in terms of OS with an acceptable toxicity, thus CCRT has become the standard management for LS-SCLC [6,7].
Etoposide plus cisplatin is the preferred chemotherapy regimen for CCRT, due to manageable toxicity when combined with TRT [8,9].
The timing of TRT in combined chemoradiotherapy has been controversial in several respects. Some argue that TRT should be started simultaneously with chemotherapy [7,10-12], while others claim that a delay of TRT (1-2 cycles) from the beginning of chemotherapy provides similar or better outcomes [13]. One rationale for the former argument is that a simultaneous start of TRT decreases the tolerance of chemotherapy, thereby reducing local relapse and distance metastasis. One disadvantage in simultaneous chemotherapy is that radiation is delivered without a prior confirming of the response to chemotherapy [10]. Several studies have reported that delaying TRT for 1-2 cycles of chemotherapy is better than a simultaneous start because the latter can increase side effects of TRT, particularly for patients with large tumors and poor lung function [14-16].
In this study it was defined as the early chemoradiotherapy when RT started within the first 3 cycles of chemotherapy. We investigated tumor response, survival, and complications in patients who received early chemoradiotherapy for LS-SCLC.
Materials and Methods
1. Patients selection
This retrospective review of clinical information was conducted between January 2006 to December 2011 in 38 patients with histopathlogically proven LS-SCLC. Among these patients, seven were excluded due to incomplete treatment, resulting in 31 patients whose data were analyzed. The 31 patients had 0-1 of the Eastern Cooperative Oncology Group performance status, had normal bone marrow, liver and renal functions and no serious disease that would impact on the treatment outcome. Patients who previously underwent chemotherapy or radiotherapy for any tumor were excluded in the present analysis.
All patients were hisopathologically diagnosed through tissue examination by bronchoscopy, percutaneous needle aspiration, and biopsy. The determination of the stage of cancer was made through physical examination and imaging studies consisting of chest X-ray, chest computed tomography (CT) scans including liver and adrenal glands and whole body bone scan, and abdominal ultrasound sonography.
2. Treatment
The initial chemotherapy regimen was administered in two cycles of etoposide (100 mg/m2) and cisplatin (60 mg/m2) every 3 weeks. This regimen was applied to all patients with the exception of four, who were administered carboplatin (area under the concentration versus time curve [AUC] 5.0, Calvert formula), instead of cisplatin with the same 100 mg/m2 of etoposide.
During CCRT, the combined chemotherapy regimen of etoposide (100 mg/m2) and cisplatin (60 mg/m2) was used in all patients every 3 weeks. After CCRT, two cycles of consolidation chemotherapy using etoposide (100 mg/m2) and cisplatin (60 mg/m2) were administrated every 3 weeks.
For TRT, 20 patients received conventional radiotherapy consisting of two parallel-opposite fields and 11 patients received 3-dimensional (3D) conformal radiotherapy. The total 50 to 60 Gy dose (median, 54 Gy) was delivered over 5 to 6.5 weeks with a daily dose of 1.8 to 2.0 Gy using 6-MV X-ray. Conventional radiotherapy was performed on the target volume including the primary tumor and mediastinal lymph node with a 1.5- to 2.0-cm margin. The first 36 Gy was delivered using parallel opposed anterior-to-posterior and posterior-to-anterior fields. After this the remaining dose was delivered to a reduced volume inclusive of the residual primary tumor and regional lymph node as a boost. In most of the boost irradiations, 3D conformal technique with three or more fields was used. 3D conformal radiotherapy of the irradiated volume was restricted to the grossly visible primary tumor and mediastinal lymph node with a 1.5- to 2.0-cm margin.
After TRT, prophylactic cranial irradiation (PCI) was applied to the patients who had a complete or partial response. PCI was delivered of 25 Gy in 2.5-Gy daily fraction dose for 10 days, 5 days per week.
3. Evaluation
Treatment results were determined via imaging tests that were performed after 4 to 6 weeks of completion of all treatments. The response to treatment was categorized according to the World Health Organization (WHO) criteria. Complete response (CR) was defined as complete disappearance of the lesions, and partial response (PR), when the lesion was shrunk by more than half. Stable disease was defined as those with tumor sizes between 50% and 125% of pre-treatment size. Progressive disease (PD) was defined when the tumor size increased by more than 25% or new lesions were identified. With regards to complications induced by the treatment, radiation-induced lung toxicity was evaluated using the Radiation Therapy Oncology Group grading system and other complications were evaluated using the Common Terminology Criteria for Adverse Events ver. 4.0.
4. Statistical analysis
OS was defined as the elapsed time from the initial treatment date to the death or to the patient's last visit. Progression-free survival (PFS) was defined as the time from the initial treatment date to the date of disease progression or the date of the patient's last visit. The initial recurrence was categorized as locoregional recurrence or distant metastasis depending on the location of the recurred lesion. Statistical analysis was performed using SAS ver. 6.02 (SAS Institute, Cary, NC, USA). PFS and OS were analyzed using the Kaplan-Meier survival method.
Results
1. Patient characteristics
The patients' characteristics are summarized in Table 1. The median age was 65 years (range, 43 to 78 years) and males were predominant. The general condition of all patients was good. Fourteen patients (45.2%) had comorbid disease, such as hypertension, diabetes mellitus, and chronic lung disease.

Patients characteristics (n = 31)
2. Tumor response and survival
Evaluation of response according to WHO criteria: CR was achieved in 11 patients (35.5%); PR in 19 (61.3%); and PD in one patient (3.2%). This provided an objective response rate (CR + PR) of 96.8% (Table 2). Figs. 1 and 2 show the OS and the PFS rates. The median survival for the 31 patients was 21.3 months. The 1-, 2-, and 3-year OS rates were 66.5%, 41.0%, and 28.1%, respectively. The median PFS was 12 months. The 1-, 2-, and 3-year PFS rates were 49.8%, 22.8%, and 13.7%, respectively.

Response
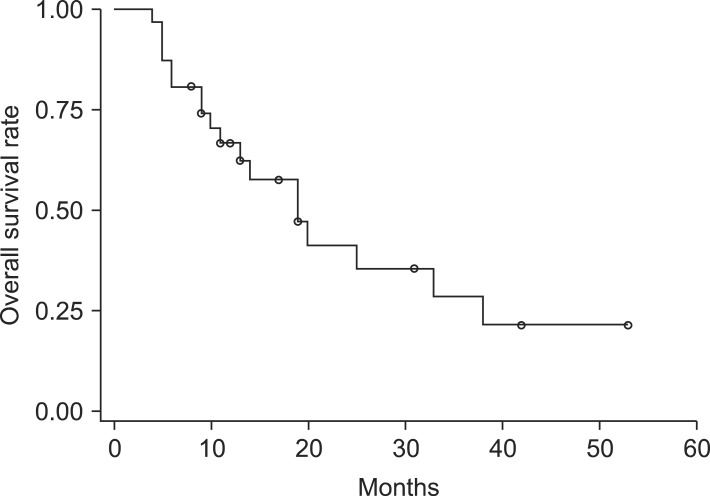
Overall survival rate.
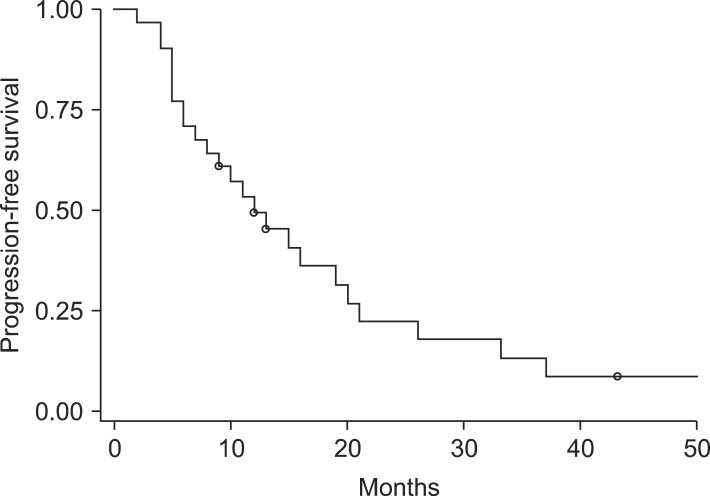
Progression-free survival.
3. Pattern of failure
Recurrences were observed in 15 of 31 patients (48.4%) as summarized in Table 3. Local recurrences were observed in nine patients (29%), distant metastasis in three patients (9.7%), and both local recurrence and distance metastasis in three patients (9.7%). Among the recurrences, brain, bone, and liver metastasis cases were five, three, and one, respectively.
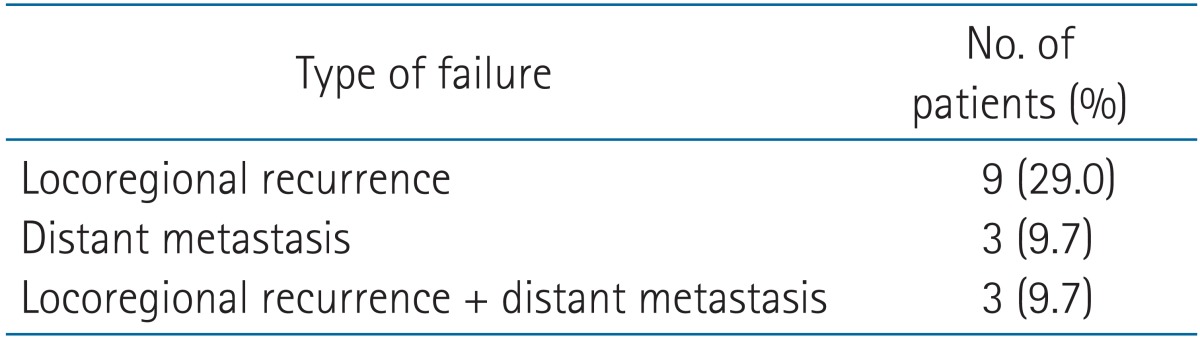
Patterns of failure
4. Toxicity
Hematologic and radiation induced toxicities are summarized in Table 4. Grade 3 or 4 hematologic toxicities were identified: leukopenia in 10 patients (32.2%), anemia in nine patients (29.0%), and thrombocytopenia in eight patients (25.8%). Grade 3 esophagitis was reported in four patients (12.9%) and radiation pneumonitis in two patients (6.4%). There were no treatment related deaths.
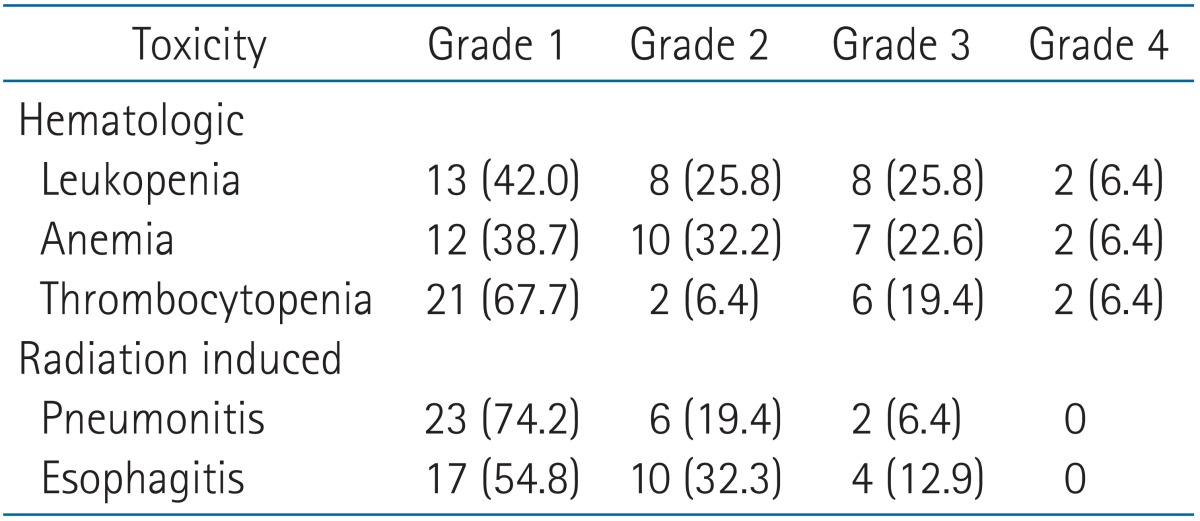
Treatment induced toxicity (n = 31)
Discussion and Conclusion
In this study we have investigated OS, PFS, and treatment-related toxicities from early CCRT following 2-cycle chemotherapy for LS-SCLC. A positive role of TRT in the treatment of LS-SCLS was clearly observed. A large percentage of the selected patients (35.5%) achieved CR after completion of CCRT; however, this was not the case when tumor response was assessed after only the initial 2-cycle chemotherapy.
Many studies have investigated the treatment timing of radiotherapy in combined chemoradiotherapy and most of these agree that CCRT is superior to sequential method [7]. It has also been reported that an early start of TRT during combined chemoradiotherapy may improve the clinical result compared with a late start. Based on previous studies recommendations advise the simultaneous start of TRT with chemotherapy [11,17]. The radiobiological rationale for this recommendation is that radiation can effectively remove the chemotherapy-resistance cells before they spread from the thorax [7,10]. The simultaneous start of radiotherapy, however, may have disadvantages. For instance, tumor sensitivity to chemotherapy cannot be confirmed at the beginning of TRT and the irradiated volume may become bigger than it would during sequential treatment. In sequential treatment the tumor is likely to shrink as a result of the chemotherapy prior to radiotherapy. The increased irradiated volume may cause an increased risk of radiation-induced complications, such as radiation pneumonitis and bone marrow suppression. Moreover, serious complications may occur when radiotherapy is combined with chemotherapy, particularly in patients with poor lung functions [18,19]. As a result of these considerations we first began the 2-cycle chemotherapy prior to radiotherapy instead of simultaneously starting both the chemotherapy and radiotherapy. We suggest that the prompt starting of chemotherapy prior to radiotherapy may help shrink tumor size, thereby helping to reduce the irradiated area in radiotherapy.
A randomized phase-III study by the Japanese Clinical Oncology Group compared the outcomes of 213 LS-SCLS patients treated by CCRT and sequential chemoradiotherapy. Patients were randomly assigned to one of two groups, a sequential treatment group where radiotherapy was administered following four cycles of chemotherapy and a concurrent start group where radiotherapy was administered prior to chemotherapy. The median survival rates were reported as 19.7 month in the sequential treatment group and as 27.2 months in the concurrent treatment group, and the 5-year survival rates were 18.3% and 23.7%, respectively. Based on the superior results of the concurrent start group, both in median survival and in 5-year survival rate, these authors also recommend the use of concurrent treatment in LS-SCLC [7].
The National Cancer Institute of Canada Clinical Trials Group performed a prospective randomized phase-III study for LS-SCLC in 380 patients, in this study results were compared between patients that received early and late radiotherapy with respect to chemotherapy [10]. Radiotherapy in the study consisted of two cycles for the early treatment group and six cycles for the late treatment group. The median survival was significantly longer in the early treatment group than that in the late treatment group (21.2 months vs. 16 months), demonstrating the superiority for the early radiotherapy in survival.
The median survival of 21.3 months in this present study is similar to that of the early treatment group (21.2 months) in the above mentioned study, demonstrating that the presented sequence of chemoradiotherapy may be acceptable compared with those in the previous chemoradiotherapy regimens.
SCLC was sensitive to both the chemotherapy and radiotherapy, but frequently relapsed mostly by local recurrence [20]. Several modifications of conventional radiotherapy to improve its effectiveness have been suggested, such as increasing the total radiation dose and using a hyperfractionation scheme that increases radiobiological effectiveness [21-23].
In another study treatment results between conventional fractionation and the hyperfractionation were compared, where a total 45-Gy dose was delivered once a day and twice a day, respectively. The result clearly showed better local control (64% vs. 48%) and 5-year survival rate (26% vs. 16%) in the hyperfractionation group [24]. In contrary, Schild et al. [15] reported that the hyperfractionation scheme did not significantly increase survival rate nor decrease local recurrence rate compared with a conventional fractionation scheme. On the other hands, in the study of Yeo et al. [25], the median survival was reported as 23 months for patients who underwent CCRT with hyperfractionated 50.4-Gy dose. Survival data from our present study are in line with these results (21.3 months vs. 23 months) even though our study employed a conventional fractionation scheme [25].
In addition, the dose escalation study was reported at the CALGB 30904 trial, where the radiation dose was escalated up to 70 Gy in 35 fractions. In this study radiation toxicity was not significantly increased and median survival was similar at 21.9 months with that reported in the hyperfractionation study [26]. In order to minimize increased risk of radiation-induced complications with the dose-escalation scheme, the CALGB 30904 trial recommended avoidance of elective nodal irradiation, determining of treatment volume using FDG-positron emission tomography combined with CT and delivering the radiation dose using advanced radiotherapy techniques, i.e., 3D conformal radiotherapy or intensity-modulated radiotherapy [27,28].
The present radiotherapy regimen with the conventional 54.0-Gy dose did not result in significant differences in tumor response and in treatment-related toxicity compared with those reported in previous studies. In order to further increase the tumor response and to decrease treatment-related toxicity, we have currently been employing the dose-escalated regimen, where the escalated 60-Gy dose is delivered to the reduced volume using 3D conformal radiotherapy or intensity-modulated radiotherapy technique.
In conclusion, in this study we have confirmed the appropriateness of early chemoradiotherapy in the management of patients with LS-SCLC and demonstrated acceptable tumor response, survival and toxicity.
Notes
No potential conflict of interest relevant to this article was reported.