Introduction
Radiotherapy (RT) is the mainstay of treatment, performed with both radical and palliative intent in patients with cervical cancer. A locally advanced disease state or disseminated systemic spread often precludes radical therapy. Even if the disease is in a curable stage, conventional radiation therapy schedules may be inappropriate in elderly patients with physical or mental impairment, and in these cases, palliative RT for symptom control is often considered [1,2]. Bleeding, pain, and vaginal discharge are the most common symptoms in patients with cancer of the uterine cervix who are treated with palliative intent [3]. Palliative RT is aimed at providing rapid symptom relief and thus improving the quality of life [4].
Previous reports have described a palliative whole-pelvic RT using single or multiple monthly 10 Gy doses. This regimen was well tolerated and effects on vaginal bleeding and discharge were seen after 2 or 3 fractions [5,6]. However, late toxicity is poorly documented and the increased risk of late toxicity is a concern because of the large fraction size and wide irradiated field. The Radiation Therapy Oncology Group (RTOG) 7905 trial adopted this monthly 10 Gy schedule concurrently with misonidazole (a hypoxic cell sensitizer), for patients with various pelvic malignancies. There was a high rate (45%) of late gastrointestinal (GI) complications, which lead to the trial being prematurely closed [7]. The RTOG prospectively investigated the use of a lower dose per fraction: a dose of 3.7 Gy (twice a day, total dose of 14.8 Gy per cycle) for 2 days repeated every month for up to three months. With this schedule, only 1 grade 3 late GI toxicity was reported among 142 patients [8].
In view of the high rate of late complications, common palliative regimens, such as 20 Gy in 5 fractions and 30 Gy in 10 fractions may be implemented. However, data regarding the clinical outcome of these regimens are limited. We used a schedule of 20 to 25 Gy in 5 Gy daily fractions using 3-dimensional conformal radiotherapy (3D-CRT) in order to achieve rapid bleeding control with less treatment-induced toxicities. The aim of the present study was to evaluate the efficacy and feasibility of short-course hypofractionated RT for the palliation of uterine cervical cancer.
Materials and Methods
Between January 2002 and June 2012, 19 patients with histologically proven squamous cell carcinoma of the uterine cervix underwent palliative RT. Two patients who discontinued RT because of pneumonia were excluded, so data for 17 patients were reviewed. The pretreatment workup comprised-pelvic and abdominal computed tomography (CT) or magnetic resonance imaging (MRI), positron emission tomography/CT, endoscopic examination, and laboratory and serum marker analysis. Patients underwent disease staging according to the 2009 classification of the American Joint Committee on Cancer staging [9]. As surgery was not performed, the disease was staged clinically.
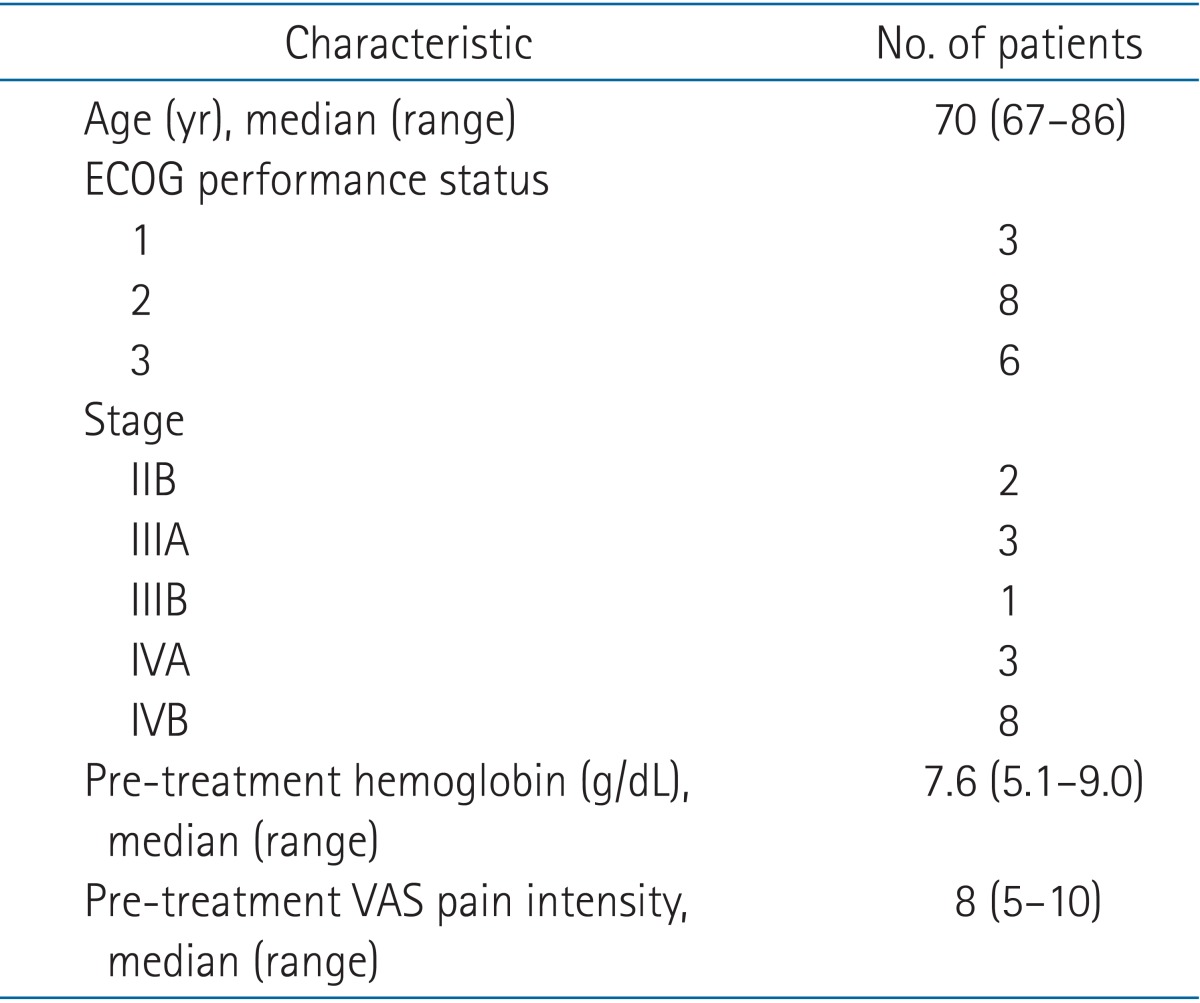
The patient characteristics are summarized in Table 1. The median age of patients was 70 years (range, 67 to 86 years). The Eastern Cooperative Oncology Group performance status was 1 (3 patients), 2 (8 patients), and 3 (6 patients), respectively. The adverse prognostic factors, due to which patients were treated with a palliative intent were as follows: disseminated disease status (8 cases), age ≥70 years (5 cases), poor physical condition (2 cases), and refusal to radical treatment (2 cases). Sixteen patients presented with vaginal bleeding, 9 with pelvic pain, and 2 with vaginal discharge. Patients with a low hemoglobin level (≤10 g/dL) were transfused with packed red blood cells before palliative RT.
Patients were treated with external beam RT. 3D-CRT was used to deliver a dose of 20 to 25 Gy (median, 25 Gy) in 5 Gy daily fractions for 5 fractions per week with 16-MV photon beams using Clinac 21EX (Varian Medical Systems, Palo Alto, CA, USA). The gross lesion responsible for vaginal bleeding or pelvic pain as identified by pelvic CT or MRI was defined as the gross tumor volume (GTV). Then the planning target volume (PTV) was defined as the GTV with the addition of a 1.0 to 2.0 cm margin, considering the setup uncertainty and organ motion [10]. The clinical target volume was not defined because treatment was delivered with a palliative intent. The treated volume was as follows: primary tumor (11 cases) and primary tumor plus metastatic pelvic lymph nodes (6 cases). All plans were generated in Eclipse (Varian Medical Systems): by using a conformal 4-field technique with 16-MV photon beams. In accordance with the International Commission on Radiation Units and Measurements rules, the PTV had to be covered by 95% to 107% of the prescribed dose. All patients were treated in the supine position with a positioning device, Kneefix (CIVCO Medical Solutions, Orange City, IA, USA) underneath the knees. Immobilization setup devices were not used because of the poor performance status and stress that would be caused to the patients.
The post-RT follow-up interval was usually 1 to 2 months for the first 6 months, and 2 to 3 months thereafter until 2 years after treatment. The median follow-up time was 12.2 months (range, 4 to 24 months). Treatment outcomes were analyzed in terms of symptom palliation and treatment related complications. Symptoms and toxicities were graded and recorded on the first day of RT and at every patient's visit during the follow-up time. The hemostatic effect was defined as vaginal bleeding cessation, or no requirement for additional transfusion or medical intervention. Pain intensity was self-assessed by patients using a visual analogue scale graded from 0 (no pain) to 10 (the strongest pain one can experience). Effective pain control was defined as a ≥50% reduction in grades. Acute and late radiation toxicities were recorded and graded according to the Common Terminology Criteria for Adverse Events ver. 4.0. Acute side effects were those appearing during treatment or within 1 month after the completion of treatment. The treatment response, disease recurrence or survival is beyond the scope of this study.
Results
The median follow-up time was 12.2 months (range, 4 to 24 months), and the median survival time was 7.8 months (range, 4 to 24 months). Treatment periods ranged from 5 to 9 days (median, 7 days). The mean GTV volume was 129.5 cm3 (range, 67.1 to 297.8 cm3). Vaginal bleeding cessation was achieved in 93.8% (15/16) of the patients. The median bleeding control time was 3 days after initiation of RT (range, 2 to 7 days). Three patients experienced vaginal bleeding relapse during the follow-up period (median elapsed time, 4 months). Reirradiation was applied to these patients with a total dose of 20 Gy in 5 fractions. One patient with persistent vaginal bleeding underwent a salvage hysterectomy. Pelvic pain was relieved in 6 of 9 patients (66.7%). During RT, non-steroidal anti-inflammatory drugs or narcotics were administered to all patients, who suffer from pelvic pain. Three out of 9 patients discontinued analgesics or were able to reduce the dose of pain medication.
Nine patients did not have any acute side effects, and 7 patients had minor GI toxicity. There was no interruption of planned RT or reduction of radiation dose due to acute toxicity. One patient complained of grade 3 diarrhea 3 days after completion of treatment, however, she showed complete symptom remission with conservative treatment. Table 2 shows the results of treatment-induced acute and late toxicities. During the follow-up period, 4 patients presented mild to moderate abdominal distension and urinary frequency. However, there was no instance of grade 3 or higher late toxicity in GI and genitourinary tracts.
Discussion and Conclusion
Many patients with uterine cervical cancer are diagnosed with disease state not suitable for radical treatment. In this situation, palliative RT for symptom control is considered. Palliative treatment aimed at a good and long-lasting relief of symptoms with a short treatment period and less toxicity. The regimen used in this study yielded good symptomatic relief in terms of vaginal bleeding (93.8%) and pelvic pain (66.7%). Moreover, significant treatment-induced acute toxicity was observed in only 1 patient (5.9%), which was alleviated after conservative medical treatment. During the follow-up period, severe late complications were not observed.
Palliative RT is frequently employed to control tumor-induced bleeding. Multiple tumor sites have been successfully treated with RT [5,6,11,12]. Vaginal bleeding is the most common symptom for which palliative RT is indicated in patients with uterine cervical carcinoma [11]. In these cases, vaginal packing and blood transfusion with hospital admission may be indicated. Some reports in the literature describe the type and dose of RT for hemostatic treatment of carcinoma of the uterine cervix (Table 3). The large single-dose schedule consists of 10 Gy fractions repeated at monthly intervals to a maximum dose of 30 Gy. This schedule has resulted in good bleeding control in approximately 90% to 100% of patients, within 24 to 48 hours of the first treatment [5,6,13-16]. The results for bleeding control (93.8%; median bleeding control time, 3 days) in this study are comparable to those reported by other series.
In the literature, the role of palliative RT for pelvic pain was unclear, with positive effects reported in approximately 22% to 63% of the cases [6,16]. This various results could be due to the different endpoints adopted in different studies. In this study, 66.7% of patients showed relief from pelvic pain. Thus, we assumed that administration of RT over a short period may be the reason for the high percentage of pain control.
The toxicity of administering a large dose per fraction is of concern because of its excessive effect on normal tissues. However, reports on the long-term outcomes of patients who receive monthly 10 Gy pelvic RT are scarce. Previous studies were retrospective and follow-up was incomplete. In addition, complications, such as fistula formation can be difficult to distinguish from disease progression. Because of the high dose delivered, the rate of late complications is high, 12% to 24% in long-term survivors, as is expected [6,7]. Moreover, a clinically significant (grade 3-4) late complication was reported in 6% to 12% of the patients [6,14,15]. In this study, only 4 patients were documented to have mild late toxicity in the form of abdominal distension, constipation, and urinary frequency. Grade 3 or higher late complications were not observed.
In the literature, the reported acute toxicity rate is usually 10% to 20%, except in the study by Onsrud et al. [14], who observed grade 1-2 acute toxicity in 44% of patients [3,15]. The treatment-induced acute toxicity of the GI and genitourinary tracts was comparable with the previously reported results. Diarrhea, nausea, abdominal distension, and urinary frequency were the main acute treatment-induced toxicities in our study. Grade 3 toxicity occurred in only 1 patient (grade 3 diarrhea) and was well controlled with conservative medical management. These results strongly suggested that a 5-Gy short-course palliative RT regimen could be also effective and safe considering both symptom palliation and complication risk.
For palliative RT, up to 3 monthly fractions of 10 Gy is most frequently described in patients with uterine cervix cancer. However, none of the previous studies provide sufficient evidence in order to determine an optimal palliative RT regimen. No comparative data are available and the previous retrospective studies have limitations. Of 8 previous studies, none compared the results of different fractionation schemes [3]. Our palliative RT scheme showed minimal toxicity compared with 10 Gy monthly fractions, especially regarding the significant late complication rate (0% vs. 6%-12%) [6,14,15]. Moreover, a reduced overall treatment period would be beneficial for patients.
A number of hypofractionated RT schemes have been described for palliation of gynecological malignancies. These regimens vary from 30 Gy in 10 fractions to shorter courses of 3.7 Gy delivered twice daily in 4 fractions, to a single doses of 8 Gy in 1 fraction [17]. Using the linear-quadratic model, total dose of 25 Gy in 5 fractions corresponds to approximately 42 to 50 Gy in 2 Gy fractions [18]. Considering the tolerance dose of normal surrounding tissues, such as the bladder, small bowel, and rectum, we assumed that this RT scheme would be safe and tolerable.
However, this study has some limitations. The poor general conditions of several patients precluded a close follow-up, and the median follow-up duration was short (12.2 months); therefore, assessment of the late complication rate could be insufficient. Moreover, this study enrolled only 17 patients, a number too small to allow generalization of the results and included a heterogeneous group of patients with various levels of tumor burden.
In conclusion, our results with palliative 3D-CRT for patients with uterine cervix cancer yielded very satisfactory clinical outcomes not only in the symptom palliation but also in the treatment related toxicity. These results were likely attributable to the relatively low fraction size and a highly conformal RT technique compared to previous studies. Different radiation fractionation schedules should be compared in order to identify an optimal fractionation schedule that will provide a sufficient degree and duration of symptom relief while causing minimal toxicity.