A comparison of preplan MRI and preplan CT-based prostate volume with intraoperative ultrasound-based prostate volume in real-time permanent brachytherapy
Article information
Abstract
Purpose
The present study compared the difference between intraoperative transrectal ultrasound (iTRUS)-based prostate volume and preplan computed tomography (CT), preplan magnetic resonance imaging (MRI)-based prostate volume to estimate the number of seeds needed for appropriate dose coverage in permanent brachytherapy for prostate cancer.
Materials and Methods
Between March 2007 and March 2011, among 112 patients who underwent permanent brachytherapy with 125I, 60 image scans of 56 patients who underwent preplan CT (pCT) or preplan MRI (pMRI) within 2 months before brachytherapy were retrospectively reviewed. Twenty-four cases among 30 cases with pCT and 26 cases among 30 cases with pMRI received neoadjuvant hormone therapy (NHT). In 34 cases, NHT started after acquisition of preplan image. The median duration of NHT after preplan image acquisition was 17 and 21 days for cases with pCT and pMRI, respectively. The prostate volume calculated by different modalities was compared. And retrospective planning with iTRUS image was performed to estimate the number of 125I seed required to obtain recommended dose distribution according to prostate volume.
Results
The mean difference in prostate volume was 9.05 mL between the pCT and iTRUS and 6.84 mL between the pMRI and iTRUS. The prostate volume was roughly overestimated by 1.36 times with pCT and by 1.33 times with pMRI. For 34 cases which received NHT after image acquisition, the prostate volume was roughly overestimated by 1.45 times with pCT and by 1.37 times with pMRI. A statistically significant difference was found between preplan image-based volume and iTRUS-based volume (p < 0.001). The median number of wasted seeds is approximately 13, when the pCT or pMRI volume was accepted without modification to assess the required number of seeds for brachytherapy.
Conclusion
pCT-based volume and pMRI-based volume tended to overestimate prostate volume in comparison to iTRUS-based volume. To reduce wasted seeds and cost of the brachytherapy, we should take the volume discrepancy into account when we estimate the number of 125I seeds for permanent brachytherapy.
Introduction
Low dose rate permanent brachytherapy is accepted as a treatment option for localized prostate cancer [1,2]. In long-term follow-up of prostate specific antigen (PSA), favorable treatment outcome has been reported [3-5]. According to prostate volume, the insertion of adequate number of 125I seeds are needed to obtain optimal coverage of prostate [6]. A preplanned technique has been widely used and patients needed to have transrectal ultrasound (TRUS) in the simulated implant position before permanent brachytherapy. Using this TRUS image, preplan was performed before brachytherapy and seeds were inserted according to the preplan in the operating room [7]. But a preplanned technique is hard to reflect the change of prostate volume between preplan TRUS and intraoperative real-time TRUS. And it is difficult to reproduce the position of patients in the operating room as the simulated position at the time of preplan TRUS. A preplanned technique also has limitation because the shape and volume of prostate can be changed when pelvic muscle is relaxed by anesthesia. As a result, the actual dosimetric finding of real-time intraoperative plan can be different with preplan [8]. Recently, real-time planning technique is accepted in many institutions. When using real-time planning technique, physicians assess shape and volume of prostate in operating room using intraoperative TRUS image just before seed insertion and make real-time virtual plan. According to this virtual plan, seeds are inserted and real-time dosimetry is carried out to ensure dose distribution of target volume [9].
Even if real-time planning technique is used, preplan image is essential. Because assessing prostate volume before brachytherapy is needed to prepare adequate number of seeds to have acceptable coverage of prostate. To obtain prostate volume, magnetic resonance imaging (MRI), computed tomography (CT) or TRUS are used and the most appropriate imaging modality to assess prostate volume is still controversial [9]. We use MRI or CT to obtain the information about stage of prostate cancer and to assess prostate volume. MRI is known to have advantage in distinguishing periprostatic tissue and prostate but it is more expensive and requires more time to scan than CT. The greater variation of contoured volume between physicians is reported for CT-based contouring than MRI-based contouring [10]. The discrepancy between preplan CT-based, preplan MRI-based and intraoperative TRUS-based prostate volume have been discussed. But the results varied among reports.
Therefore, we retrospectively reviewed the prostate volumes obtained from preplan CT, preplan MRI and intraoperative TRUS to compare the degree of difference between imaging modalities. And we calculated the number of seeds needed for brachytherapy according to prostate volume.
Materials and Methods
Between March 2007 and March 2011, among 112 patients who underwent permanent brachytherapy with 125I, 60 image scan of 56 patients who underwent preplan CT or preplan MRI within 2 months before brachytherapy was retrospectively reviewed. 26 patients underwent only MRI scan and 26 patients underwent only CT scan. 4 patients underwent both CT and MRI scan. 21 cases received total androgen suppression [luteinizing hormone releasing hormone (LHRH) agonist and antiandrogen] and 29 cases received only antiandrogen (biglutamide) as neoadjuvant hormone therapy (NHT). 10 cases did not receive NHT. Twenty-four cases with preplan CT and 26 cases with preplan MRI received NHT. The median duration of NHT after preplan image acquisition was 17 days (range, 2 to 35 days) for cases with preplan CT and 21 days (range, 2 to 46 days) for cases with preplan MRI. And the median duration of overall NHT before brachytherapy was 22 days (range, 4 to 100 days) for cases with preplan CT and 25 days (range, 7 to 46 days) for cases with preplan MRI.
Low risk group was defined as T1-T2a, Gleason score ≤ 6 and PSA < 10 ng/mL. Intermediate risk group was defined as T2b-T2c or Gleason score 7 or PSA 10-20 ng/mL. High risk group was defined as T3-T4 or Gleason score 8-10 or PSA > 20 ng/mL (Table 1).
Patient characteristics
One radiation oncologist contoured prostate on preplan CT or preplan MRI image scanned as 5 mm slice thickness using treatment planning system iPlan 3.0 (BrainLAB AG, Feldkirchen, Germany). The prostate volume was delineated on all slices from the base of bladder to the superior border of urethral sphincter muscle and seminal vesicle did not included. For real-time imaging, intraoperative TRUS image was captured with Pro Focus 2202 (BK Medical, Herlev, Denmark, 2008) at 5 mm interval from fundus to apex of prostate. These images were sent to the Strata Volume Plan (Rosses Medical System, Columbia, MD, USA) to delineate the prostate volume acquired by TRUS. The prostate volume was delineated from apex to fundus of prostate on every slice in operating room after capturing the TRUS image (Fig. 1). CT scan was conducted with the Somatom sensation 16 (Siemens AG, Forchheim, Germany, 2004) and MRI scan was conducted with the Signa HDxt 3.0T (GE Healthcare, Waukesha, USA, 2005). Some patients underwent CT or MRI scan at outside hospital and these images were used if appropriate. A comparison was made between preplan CT volume and the intraoperative TRUS volume for 30 cases which had preplan CT. And a comparison was made between preplan MRI volume and the intraoperative TRUS volume for other 30 cases which had preplan MRI. The Pearson correlation coefficient was used to evaluate the correlation between preplan image-based volume and intraoperative TRUS-based volume. And prostate volume obtained from preplan image and intraoperative image was compared by paired-sample t-test with two-tailed significance. And the actual difference of prostate volume measured by different modalities was calculated. Independent sample t-test was performed to assess the difference between the ratio of measured prostate volume by preplan CT/intraoperative TRUS and preplan MRI/intraoperative TRUS. Analysis was performed using SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA).
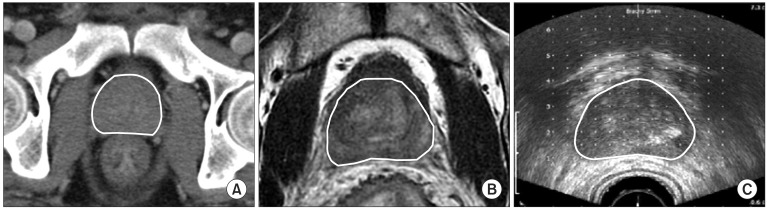
Contouring of prostate based on different imaging modality. 3 images of one patient were used to contour prostate. (A) Computed tomography-based contouring of prostate. (B) Magnetic resonance imaging-based contouring of prostate. (C) Transrectal ultrasound-based contouring of prostate.
And we retrospectively conducted intraoperative TRUS-based planning for every enrolled patients according to the guidelines of Chauveinc et al. [11] and Salembier et al. [12] to assess the required number of seeds for optimal dose coverage. Chauveinc et al. [11] reported that D90 (the dose that covers 90% of the prostate volume) more than 175 Gy and V100 (the percentage of volume that receives the prescribed dose) more than 99.95% guaranteed the adequate dose coverage in postimplant-dosimetry. Salembier et al. [12] recommended about target delineation and dose prescription in a supplement to the ESTRO/EAU/EORTC recommendations on prostate brachytherapy. The visible contour of the prostate expanded with a three-dimensional volume expansion of 3 mm becomes clinical target volume in the recommendation. And clinical target volume is used as planning target volume. And the V100 must be at least 95%. Consequently, D90 will be larger than the prescription dose. And the V150 (the percentage of volume that receives 150% of the prescription dose) should be equal to or less than 50%. Strata Volume Plan does not include option for 3-dimensional volume expansion. So we manually drew clinical target volume with 3 mm margin around gross target volume on each slice. Volume expansion to superior and inferior direction was not performed. We retrospectively planned to fulfill these recommendations about clinical target volume. The activity of seed was corrected as 0.35 mCi for all cases. And we estimated the difference of seed numbers according to preplan image-based prostate volume and intraoperative TRUS-based prostate volume.
Results
1. The difference between preplan image-based prostate volume and intraoperative TRUS-based prostate volume
The mean difference in volume between the preplan CT and intraoperative TRUS was 9.05 mL. And the mean difference in volume between the preplan MRI and intraoperative TRUS was 6.84 mL. The mean prostate volume was 34.16 mL (range, 20.19 to 54.55 mL) in preplan CT image and 25.11 mL (range, 12.78 to 45.44 mL) in intraoperative TRUS image. Prostate volume measured by intrraoperative TRUS was larger than volume by preplan CT in 2 cases. The difference in volume for case 1 was 0.62 mL and 0.17 mL for case 2. The mean prostate volume was 27.84 mL (range, 14.96 to 40.28 mL) in preplan MRI image and 21.00 mL (range, 11.28 to 33.23 mL) in intraoperative TRUS image. The prostate volume was roughly overestimated by 1.36 times with preplan CT and by 1.33 times with preplan MRI. Two-tailed paired T test was conducted between preplan CT-based volume and intraoperative TRUS-based volume and a statistically significant difference were found (p < 0.001). Two-tailed paired t-test was conducted between preplan MRI-based volume and intraoperative TRUS-based volume and a statistically significant difference were also found (p < 0.001). Preplan MRI volumes and preplan CT volumes were correlated with intraoperative TRUS volumes (R = 0.894, p < 0.001 for preplan MRI and R = 0.871, p < 0.001 for preplan CT) (Fig. 2). The degree of volume reduction did not have statistically significant difference according to preplan imaging modality (p = 0.153).
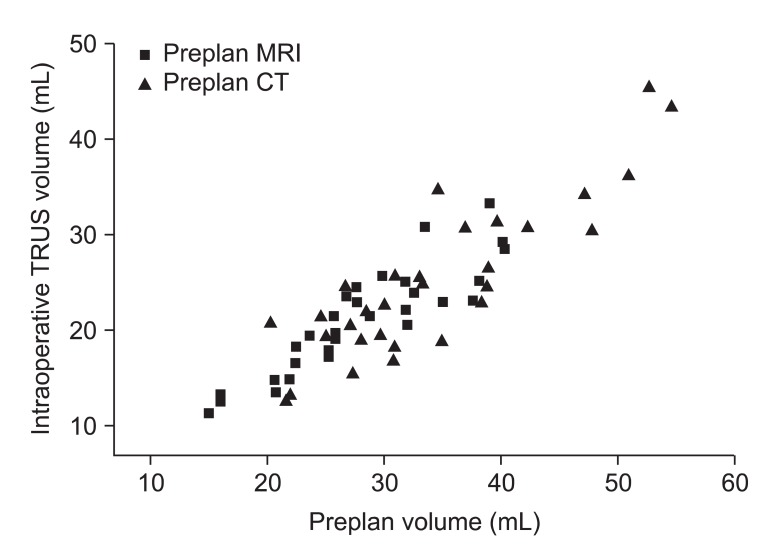
Correlation of prostate volume with preplan computed tomography (CT) or preplan magnetic resonance imaging (MRI) and intraoperative transrectal ultrasound (TRUS). Correlation of prostate volume between image modalities was measured by comparing preplan CT or preplan MRI-based volume and intraoperative TRUS-based volume. Pearson's correlation coefficient was 0.871 for CT group (p < 0.001) and 0.894 for MRI group (p < 0.001).
When subgroup analysis was conducted for 34 cases which started NHT after obtaining preplan CT or preplan MRI scan, the prostate volume was roughly overestimated by 1.45 times for 15 cases with preplan CT and by 1.37 times for 19 cases with preplan MRI. The median duration of NHT for cases with preplan CT and preplan MRI was 22 days (range, 4 to 35 days) and 21 days (range, 7 to 46 days). The degree of volume reduction did not have statistically significant difference between preplan CT and preplan MRI (p = 0.148). And the degree of volume reduction did not have statistically significant difference between 34 cases which started NHT after obtaining preplan CT or preplan MRI scan and 10 cases which did not receive NHT (p = 0.095).
2. The number of seeds needed for permanent brachytherapy according to prostate volume
We conducted retrospective planning with intraoperative TRUS image to obtain information for number of seeds to prescribe 145 Gy with optimal dose coverage according to clinical target volume. And the required number of seeds was recorded for each patient.
The median number of seeds with 0.35 mCi activity was 58 (range, 45 to 60) for gross prostate volume less than 15 mL to ensure dosimetric coverage of clinical target volume; 68 (range, 64 to 82) for 15.0-19.9 mL, 86 (range, 77 to 92) for 20.0-24.9 mL, 91 (range, 85 to 92) for 25.0-29.9 mL, 102 (range, 85 to 108) for 30.0-34.9 mL, 116 (range, 114 to 122) for 35.0 mL and more, respectively (Table 2, Fig. 3).

Modified seeda) counts according to retrospective plan using intraoperative transrectal ultrasound

The number of required seeds in retrospective plan according to prostate volume. The number of seeds required for dose coverage according to prostate volume in retrospective plan was represented. TRUS, transrectal ultrasound.
We calculated the difference of required seed numbers between preplan image-based volume and intraoperative TRUS-based volume for each case. We adopted the number of seeds from retrospective planning as the actual number of seeds needed for brachytherapy. And the required number of seeds for preplan image-based volume was calculated approximately using the previously stated median number of seeds according to the volume. In the case of preplan CT, the median difference of seed number was 11 (range, -12 to 38) and mean difference of seed number was 13. For preplan MRI, the median difference of seed number was 15 (range, -3 to 33) and mean difference of seed number was 15. If we use the preplan CT or preplan MRI volume to assess the required number of seeds without modification, the median number of wasted seeds is 13.
Discussion and Conclusion
Real-time planning technique using intraoperative TRUS is adopted as an effective method to reflect real-time prostate shape and volume. In this technique, preplan is done just before seed insertion using real-time intraoperative TRUS image at operating room and according to preplan, seeds are inserted to prostate [9]. But it is necessary to predict the intraoperative volume of prostate approximately before preparing 125I seeds for brachytherapy to reduce number of wasted seeds.
Fogh et al. [9] reported that the mean difference between preplan TRUS-based volume and intraoperative TRUS-based volume was 3.59 mL and the correlation coefficient was 0.84. The mean difference between preplan CT-based volume and intraoperative TRUS-based volume was 5.2 mL and the correlation coefficient was 0.82. Tanaka et al. [13] reported that preplan CT-based prostate volume is 1.17 times larger than preplan TRUS-based prostate volume and preplan MRI underestimated prostate volume 0.73 mL in comparison to TRUS-based volume. Smith et al. [14] demonstrated the average ratio for CT/MR volumes, TRUS/MRI volumes, CT/TRUS volumes were 1.16, 0.90 and 1.30, respectively.
The previously stated studies reported that CT overestimated prostate volume than TRUS and MRI underestimated prostate volume than TRUS or demonstrated similar volume with TRUS. But in this study, both CT and MRI overestimated prostate volume in comparison to TRUS.
A large part of studies have been reported that the CT-based prostate volume was larger than the MR-based prostate volume. Roach et al. [15] reported that the volume of prostate from 10 patients who had both CT scan and MRI scan was compared and CT-based volume was 1.32 times (range, 1.05 to 1.63 times) larger than MRI-based volume. A study by Rasch et al. [16] compared CT-based volume and MRI-based volume from 18 patients delineated by 3 radiation oncologists for all images. And CT volumes were larger than MRI volumes in 52 of 54 delineations. And CT volumes were 1.4 times larger than MRI volumes on average. Kagawa et al. [17] reported the mean CT-based prostate volume and MRI-based prostate volume was 63.0 (+/- 25.8) cm3 and 50.9 (+/- 22.9) cm3, respectively.
On the other hand, Parker et al. [18] reported that the average ratio between the CT and MRI volumes was 1.02 and Prete et al. [19] reported that MRI overestimated prostate volume by an average of 9.1% than CT. Parker et al. [18] explained the similarity in prostate volume measured by CT and MRI with various reasons. The investigators knew that CT tended to overestimate volume in comparison to MRI and contouring was done considering sagittal and coronal reconstructed images. Prete et al. [19] suggested that interobserver variation which was known to happen in CT-based contouring more than MRI-based contouring might be the reason for the opposed result. In this study, only 4 patients obtained both CT and MRI scan and the mean ratio of CT/MRI volume was 1.1. In majority of cases, we could not compare CT-based volume and MRI-based volume directly in the same patient, but the difference in ratio between CT/TRUS volume and MRI/TRUS volume was less than previous reports. We also contoured prostate on axial image and modified the contour according to coronal and saggital reconstruction images. And this contouring method might affect the result in our study as stated before by Parker et al. [18].
The limitation of this study is that not all patients had both CT and MRI scan. So direct comparison between CT-based volume and MRI-based volume was not possible for all cases and we just evaluated the difference between preplan CT or preplan MRI-based volume and intraoperative TRUS-based volume.
In this study, 50 of 60 cases received NHT and it might affect the ratio of prostate volume between preplan image and intraoperative image. In addition, variability of duration and regimen of NHT might cause biased result. The duration of NHT after image scan (p = 0.055) and overall duration of NHT (p = 0.859) did not have statistically significant difference between preplan CT and preplan MRI group. But in each group, the duration of NHT was not consistent among cases. The duration of NHT after image scan was median 17 days (range, 2 to 35 days) for cases with preplan CT and 21 days (range, 2 to 46 days) for cases with preplan MRI. Langenhuijsen et al. [20] reported that 31% reduction of prostate volume occurred during the first 3 months after initiation of NHT. During the next 3 months, 9% reduction of prostate volume was reported. And after that, no significant change of prostate volume was measured. To our knowledge, there is no report about the extent of prostate volume reduction for less than 3 months duration of NHT. So it is hard to make an accurate estimate of the extent of volume reduction by NHT for this study. Prospective study comparing the volume of prostate between CT and MRI in the same patient is needed under the control of NHT regimen and duration to confirm the volume discrepancy between image modalities and the effect of NHT on volume reduction. After that, we can make an accurate estimate of the number of seeds needed for dose coverage according to preplan image-based prostate volume.
Preplan CT volume and preplan MRI volume have a tendency to overestimate prostate volume in comparison to intraoperative TRUS volume. To reduce wasted seeds and cost of the brachytherapy, we should take the volume discrepancy into account when we estimate the number of 125I seeds for permanent brachytherapy.
Notes
No potential conflict of interest relevant to this article was reported.