Introduction
Salivary gland cancers represent 3%-6% of all head and neck cancers in adults [1]. Salivary duct carcinoma (SDC) is a rare type of salivary gland cancer and is recognized as an aggressive malignancy. Because it is rare, no prospective studies on SDC have been published and only a few retrospective reports on 10 to 50 patients are available [2,3,4,5]. In Korea, previous research has included a retrospective study of 35 patients treated with surgery and adjuvant postoperative radiotherapy and case reports of patients with SDC [6,7,8,9,10].
SDC occurs mainly in the parotid gland and has poor prognosis and frequent local and distant failures. According to some reports, most patients with SDC die within three years [1,4]. Five-year overall survivals are reported to be 42% for stage I, 40% for stage II, 30% for stage III, and 23% for stage IV disease [4]. In a review of literature by Hosal et al. [3], local recurrence was experienced by 15%-55% of patients and distant metastasis by 33%-62%.
Because of the rarity of the disease, results regarding the treatment of SDC are limited. This report is a retrospective study of SDC patients at a single institution in Korea who were treated with surgery and postoperative radiotherapy.
Materials and Methods
1. Patient eligibility and characteristics
A retrospective analysis of all patients with SDC was performed at our institution. A list of SDC patients between January 2005 and December 2012 from an institutional cancer registry identified 16 patients. Patients who had salivary gland surgery and histologically proven SDC were included in analysis. All patients received postoperative radiotherapy; patients who failed to finish scheduled radiotherapy were excluded. We excluded 1 patient who received 16.2 Gy of radiotherapy because patients who fail to finish the scheduled radiotherapy were excluded from analysis. He received salvage re-irradiation after recurrence in postoperative tumor bed and successfully achieved disease control, but lung metastasis occurred later.
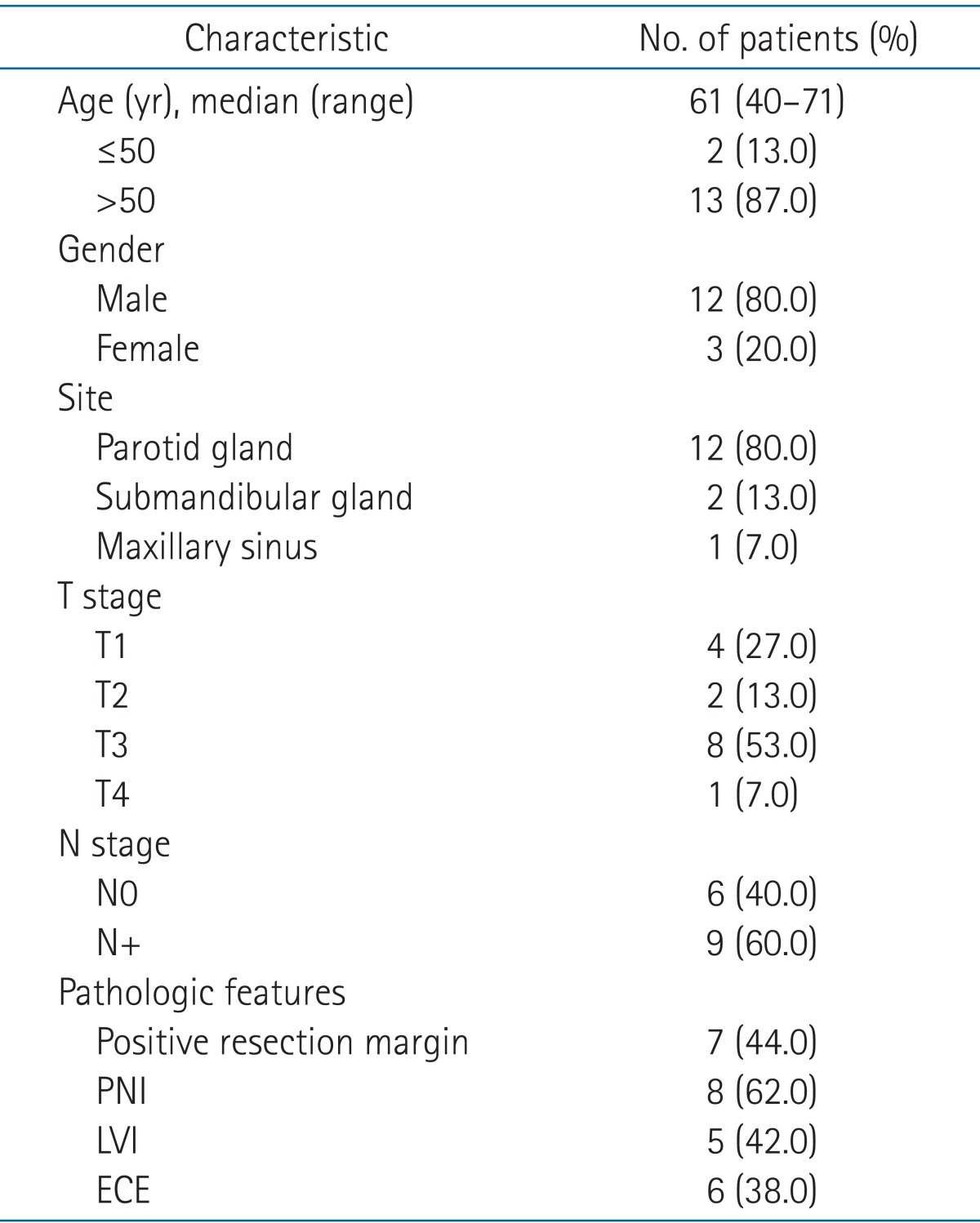
Of the 16 patients identified, 15 eligible patients were analyzed. The characteristics of the 15 patients are in Table 1. The median age was 61 years (range, 40 to 71 years) with 13 (87%) older than 50 years, and 12 patients (80%) were men. Twelve patients (80%) had a tumor in the parotid gland, 2 (13%) in the submandibular gland, and 1 (7%) in the maxillary sinus. Nine patients (60%) had T3 or T4 disease, and 9 (60%) had positive nodal disease. Seven patients (44%) had a positive resection margin, 8 (62%) had perineural invasion, 5 (42%) had lymphovascular invasion, and 6 (38%) had extracapsular extension of metastatic lymph nodes.
2. Pretreatment evaluation
Pretreatment evaluation included a complete history and physical examination. Laboratory studies included a complete blood cell count and serum chemistry profile. For stage workup, patients underwent imaging studies, such as computed tomography (CT) and/or magnetic resonance imaging (MRI). Positron emission tomography, whole body bone scans, and chest CT were performed for systemic evaluation.
3. Treatment details
Patients received surgery and postoperative radiotherapy. Postoperative radiotherapy was administered after wound recovery from surgery using ≥6 MV photons generated by a linear accelerator. Either 3-dimensional conformal radiotherapy (3D-CRT) or intensity-modulated radiotherapy (IMRT) was used. Contrast-enhanced CT simulation with thermoplastic device was mandatory and a mouthpiece to remove the tongue from the radiation field was used according to the radiation oncologist's preference. Gross tumor volume (GTV) included residual tumor volume and metastatic lymph nodes. Clinical target volume (CTV) was defined as GTV plus a 2-cm margin or postoperative tumor bed plus a 1-cm margin and encompassed the elective nodal area. In all patients, elective nodal irradiation (ENI) target volume was the nodal areas of the operated neck including level II, level III, and level IV neck nodes. We used 3D-CRT, multifield technique, and cone-down technique. Total radiation dose was 63 Gy if the patient had risk factors, such as gross residual tumor or extracapsular extension of metastatic lymph nodes; if a patient had no risk factors, the total radiation dose was 59.4 Gy. For N0 patients, after a dose of 45 Gy in 25 fractions, CTV was reduced to the postoperative tumor bed plus a 1-cm margin and ENI of level II and level III to deliver an additional boost dose of 14.4 Gy. Using IMRT, a simultaneously integrated boost technique was used so the GTV received a dose of 2.12 Gy per fraction. CTV1 encompassed the elective nodal area of level II and level III received 1.8 Gy per fraction; CTV2 encompassed the elective nodal area of level IV and received 1.7 Gy per fraction. The total fraction number of IMRT was 30. Total doses were 63.6 Gy for GTV, 54 Gy for CTV1, and 51 Gy for CTV2. Total IMRT dose was similar to total dose of 3D-CRT in biologically equivalent doses. CTV was modified to reduce the dose to organs at risk, such as the spinal cord, optic apparatus (optic nerves and chiasm), mandible, pharynx, larynx, and esophagus. The maximal dose constraints were below 45 Gy for the spinal cord, below 55 Gy for the optic apparatus, and below 70 Gy for the mandible. Other organs at risk, such as the larynx, pharynx, and esophagus, were also delineated and set for doses as low as possible. For the planning target volume, a 0.3-cm margin was applied to the CTV considering patient motion and daily setup error.
Four patients received concurrent weekly chemotherapy of cisplatin (40 mg/m2). One patient aged 70 years received a dose of 25 mg/m2 because he had poor general performance status. Cisplatin was administered on day 1. Indications of chemotherapy were gross residual tumor, positive resection margin, and extracapsular extension of metastatic lymph nodes. After scheduled postoperative radiotherapy, no adjuvant chemotherapy was given.
4. Follow-up and response assessment
Each patient was examined weekly to monitor treatment-related toxicities through all phases of treatment or more often if clinically indicated. After radiotherapy completion, patients visited the hospital every 3 months for the first 2 years, every 6 months for the next 3 years, and annually thereafter. Follow-up studies consisted of blood tests including complete blood count, serum chemistry profile, and imaging studies, such as MRI or CT to assess treatment response. Response was evaluated using the Response Evaluation Criteria in Solid Tumors after completion of the therapy. Acute toxicities were recorded according to the National Cancer Institute's Common Toxicity Criteria ver. 3.0.
Local failure was defined as increase in size of the residual tumor or a new lesion in the postoperative tumor bed, or failure in the radiation field. Regional failure was defined as the occurrence of a new lesion in the regional lymph node area or soft tissues adjacent to the nodal area. Distant failure was defined as metastatic lesion in distant organs, such as the lung, mediastinum lymph node, or brain.
5. Statistical analysis
All statistical analysis used SPSS ver. 20.0 (IBM, Armonk, NY, USA). Locoregional failure-free survival (LRFFS), distant failure-free survival (DFFS), progression-free survival (PFS), and overall survival (OS) were calculated from the date of diagnosis to the event and were plotted using the Kaplan-Meier method. Differences in survival between risk factors were tested using a log-rank test. A p-value <0.05 was considered statistically significant.
Results
1. Treatment characteristics
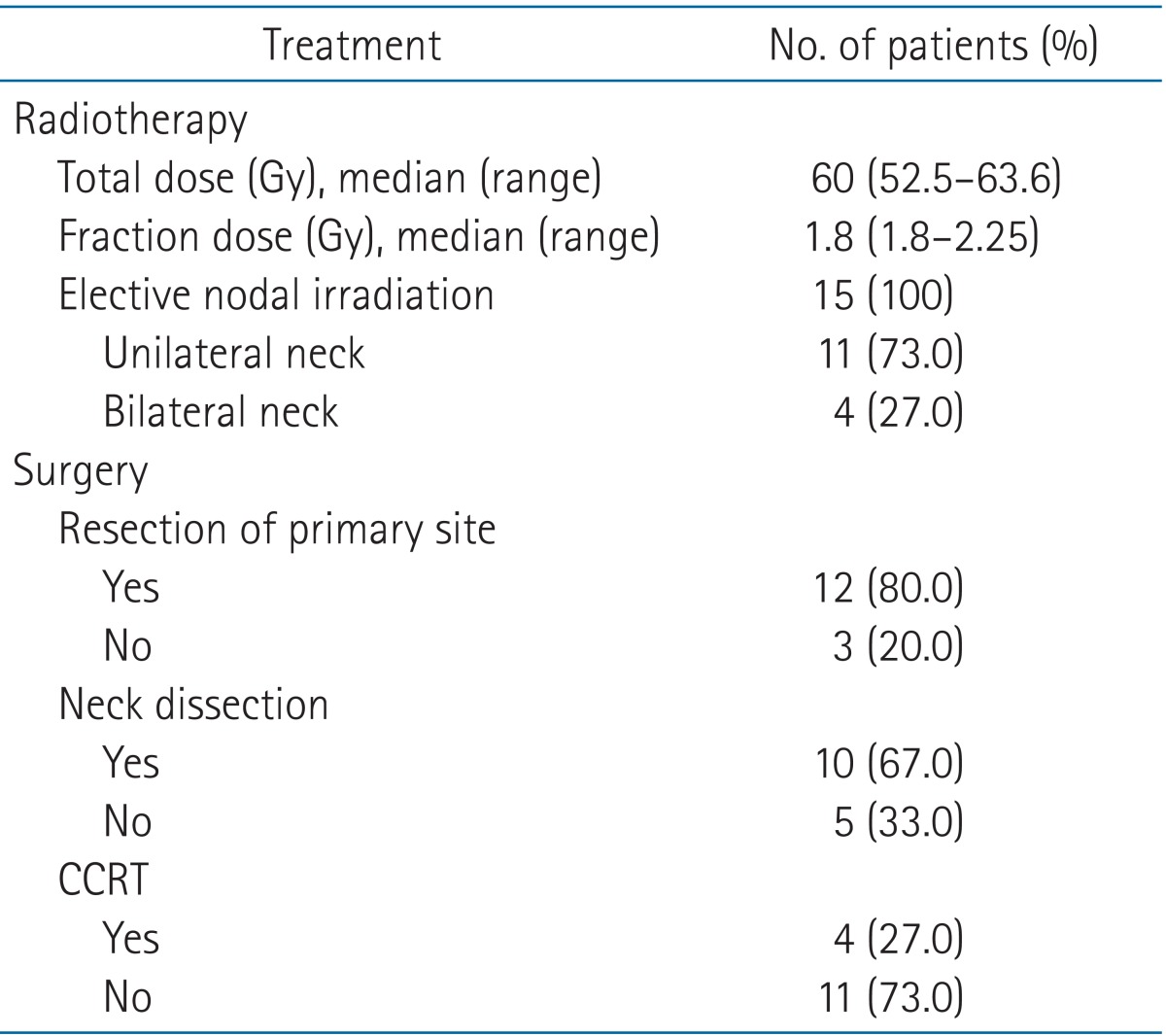
Treatment characteristics of patients are summarized in Table 2. Median total radiotherapy dose was 60 Gy (range, 52.5 to 63.6 Gy) and median fractional dose was 1.8 Gy (range, 1.8 to 2.25 Gy). All patients received postoperative tumor bed irradiation and elective nodal irradiation of level II, III, IV; 11 patients (73%) were treated with unilateral neck irradiation and 4 (27%) were treated with bilateral neck irradiation. Total resection of the primary site was performed for 12 patients (80%), and 3 patients (20%) underwent tumor resection only. Neck dissection was done for 10 patients (63%) and 4 (25%) underwent weekly cisplatin-based concurrent chemoradiotherapy. Of 10 patients with neck dissection, 7 received modified radical neck dissection, 2 had supraomohyoid neck dissection, and 1 had lateral neck dissection.
2. Survival analysis
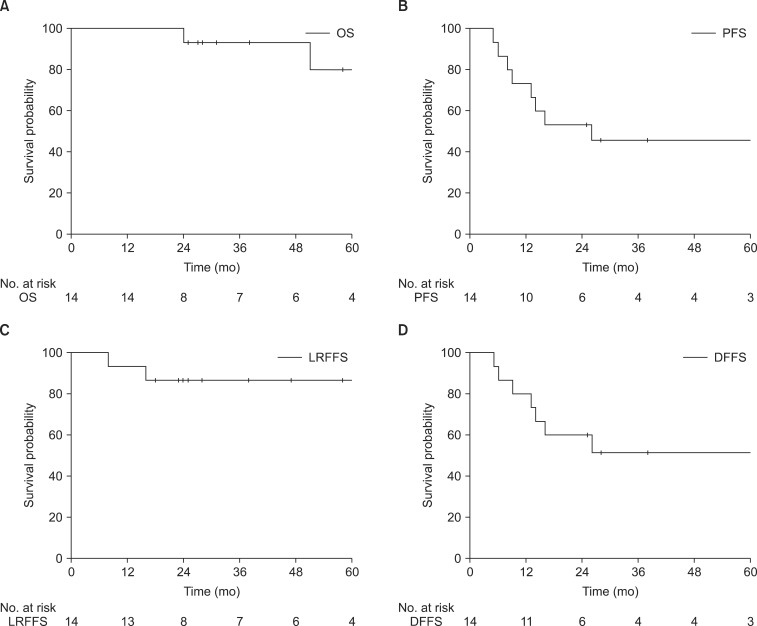
The median follow-up time was 38 months (range, 24 to 105 months) for all patients and 38 months (range, 25 to 105 months) for patients who were still alive at the time of analysis. Fig. 1 shows survival analysis for SDC patients. Four-year rates were 86% for LRFFS, 51% for DFFS, 46% for PFS, and 93% for OS.
3. Patterns of failure and risk factors for survival and toxicity
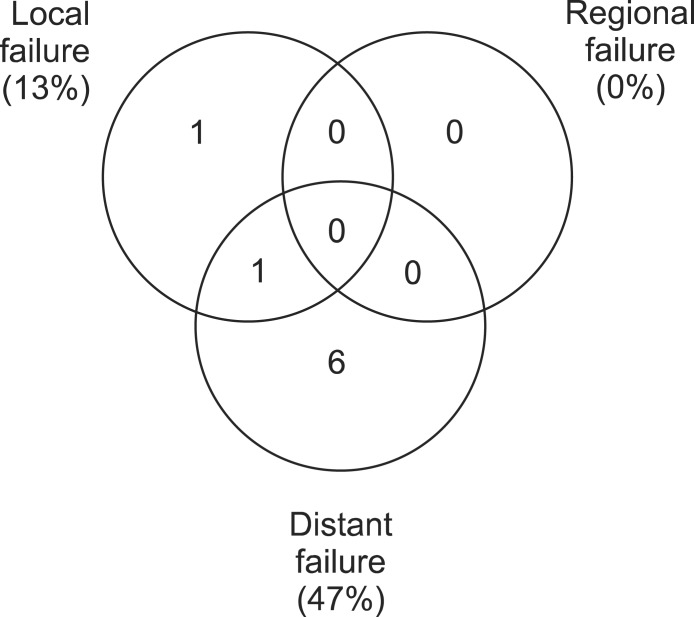
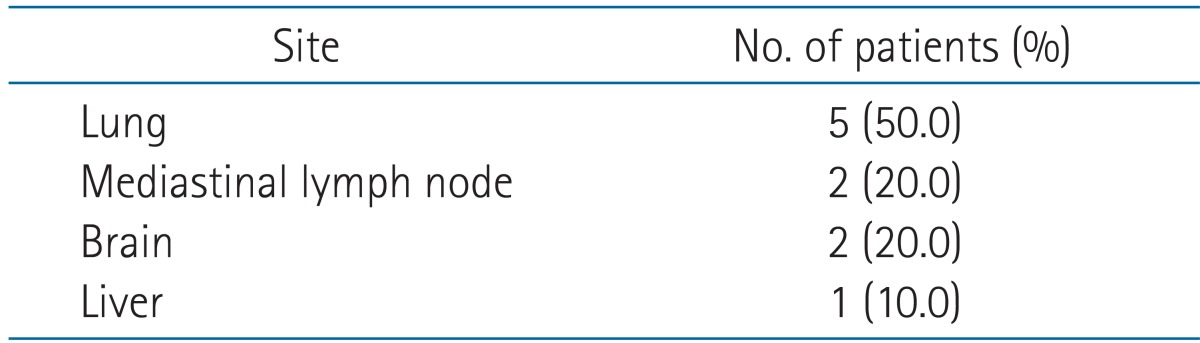
Patterns of failure are in Fig. 2. Local failure was observed for 2 patients (13%), and distant failure was observed for 7 (47%). In contrast to the relatively high rate of distant failure, local or regional failure was less common. Of 2 patients who had local failure, one had SDC at the parotid gland and received total parotidectomy. Pathologic stage was pT3N0M0 with positive perineural invasion. The patient had supra-auricular skin recurrence at 8 months after postoperative radiotherapy, apparently within the radiotherapy field. Retrospective review of the radiation field indicated that the radiation dose to the superficial skin was insufficient. After wide resection of the skin at the recurrent disease and ear covering with an anterior lateral thigh flap, the patient recovered and had no evidence of disease at last follow-up. Another patient who initially had a tumor at the left parotid gland with pathologic stage pT3N2bM0, perineural invasion, lymphovascular invasion, and extracapsular extension of metastatic lymph nodes experienced local recurrence in the internal auditory canal. Recurrent disease at the internal auditory canal occurred just outside the border of the radiotherapy field. The patient had synchronous local and distant failure with lung metastasis. Although salvage re-irradiation was attempted, the patient died from lung metastasis progression. Table 3 shows distant failure sites. The lung was the most commonly involved distant metastasis site.
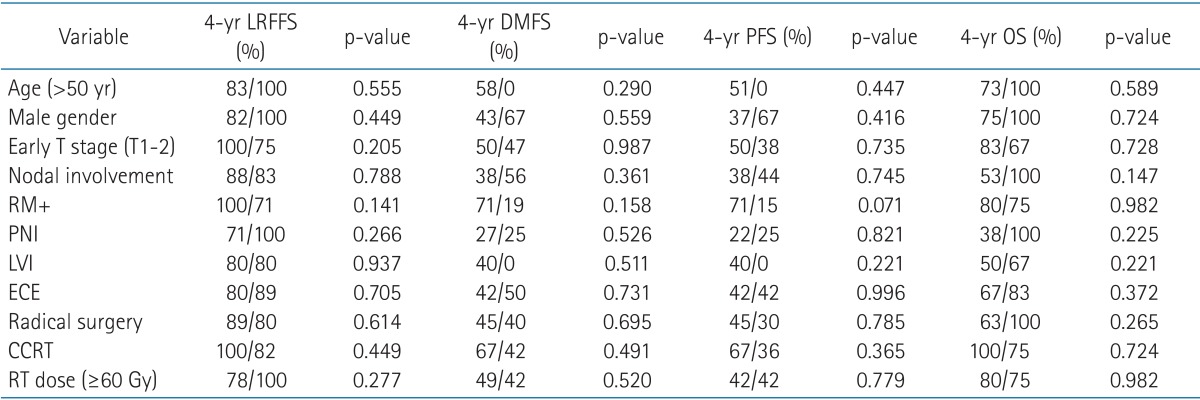
Risk factors for survival are summarized in Table 4. Positive resection margin showed only a trend toward improved PFS (71% vs. 15%, p = 0.071). Only 2 patients had distant metastasis with positive resection margins, whereas 2 had local failures and 4 had distant metastases with negative resection margin. Age, sex, T stage, N stage, perineural invasion, lymphovascular invasion, extracapsular extension, radical surgery, concurrent chemoradiotherapy, and radiotherapy dose were not associated with LRFFS, DMFS, PFS, or OS.
No grade 3 or 4 acute toxicities were observed. The most frequent toxicities were grade 2 oral mucositis and grade 2 radiation dermatitis.
Discussion and Conclusion
SDC was first described by Kleinsasser and his colleagues in 1968. SDC is a high-grade tumor and occurs at the ductal epithelium of the salivary gland. Histologically, SDC is indistinguishable from ductal carcinoma of the breast [11]. The standard treat ment for SDC is surgical resection with postoperative radiotherapy. However, many investigators noted that distant metastasis is a major clinical problem and most patients die from disseminated disease. Hosal et al. [3] reported that 43% of patients experience distant metastasis and 21% experience local recurrence after surgery and postoperative radiotherapy. Brandwein et al. [12] reported that 54% of patients experience distant metastasis and 45% experience local recurrence. Guzzo et al. [13] reported that, with combined surgery and radiotherapy, 65% of patients achieve local-regional control, but 46% experience distant failures. Our results showing 14% local recurrence and 53% distant metastasis were comparable to other studies, and our patients showed durable local-regional control. However, high rates of distant metastasis are inevitable with current management.
Considering that SDC is a very rare tumor, only limited data are available on its biological behavior and immuno-histochemical characteristics. Molecular studies show frequent overexpression of human epidermal growth factor receptor 2 (HER2) [14]. Because of the high incidence of HER2 overexpression, some studies reported on trastuzumab-based therapy for in SDC. Nabili et al. [15] reported that, of 7 patients with HER2-positive SDC, 3 demonstrated a good response to chemotherapy in combination with trastuzumab. Perissinotti et al. [2] studied the role of trastuzumab in SDC management, and showed that high-risk patients receiving trastuzumab-based chemotherapy had no tumor recurrence. We could not perform further investigations on molecular markers, such as HER2, because our study was retrospective.
Our study had limitations of retrospective study design and a small number of patients. Because of these limitations, we could not find risk factors that were statistically significant. Kim et al. [10] reported that lymphovascular invasion and perineural invasion are significant prognostic factors for SDC. We showed only a trend for improved PFS with positive resection margins. As tumors with positive resection margins after surgery tend to easily recur, our results seemed to be unusual. We reviewed the relationship between radiation dose and resection margin and target volume. No total radiation dose differences were seen in CTV between patients with positive resection margins and negative resection margins. However for target volume, wide generous margins were applied to patients with positive resection margins. Patients who were treated with generous margins because of positive resection margins experienced no local failures, but patients with negative resection margins experienced 2 local failures. No studies have reported an adequate target volume for radiotherapy for SDC patients. According to Shinoto et al. [16], for patients with positive perineural invasion, CTV of involved cranial nerves and corresponding parts of the skull base was appropriate. In our study, CTV did not include involved cranial nerves or corresponding parts of the skull base. One patient had local recurrence in the internal auditory canal. Since he had positive perineural invasion, local control was achieved with CTV that included the involved cranial nerve. In addition, no patients had regional nodal failure when treated with elective nodal irradiation. The appropriate target volume for postoperative radiotherapy should be investigated for SDC.
Our findings showed very favorable results for locoregional control when treating SDC patients with surgery and postoperative radiotherapy. Based on our results and evidence from other reports, distant metastasis remains a major challenge of this aggressive disease. Further investigation is needed to explore effective systemic treatments for patients with high risk factors for distant metastasis.