Introduction
Kaposi's sarcoma (KS) can be classified into 4 categories by the region, race, immunologic status (e.g., history of kidney transplantation), and human immunodeficiency virus (HIV) infection. Median survival ranges from several weeks to years according to the classification [1]. Among them, non-HIV associated KS (NAKS) has relatively indolent disease course. In the review of classic KS treatment, size reduction of 50% or more was achieved in 62% treated with intralesional vincristine, 50-90% with interferon-α2, 56% with imiquimod, 25% with nicotine patches, and complete remission was achieved in 60-93% of lesions with radiotherapy (RT) [2]. In 1994, Chang et al. [3] found that KS was related to human herpesvirus-8 (HHV-8), also known as Kaposi's sarcoma-associated herpesvirus (KSHV). The rate of KSHV infection varies among geographic regions. The infection rate is high in the Sub-Saharan Africa or Mediterranean country and is associated with high prevalence of the KS whereas infection rate is less than 10% in North America or Asia including South Korea. Underlying conditions causing immunodeficiency as HIV or transplantation are well known factors for development of KS in KSHV infected patients. Additionally, Goedert et al. [4] reported that steroid medication has positive and cigarette smoking has negative additive effect to development of KS.
Few randomized studies have been performed for NAKS for its rarity and indolent nature, therefore standard treatment has not been established. Limited numbers of asymptomatic lesions can be closely observed, and symptomatic lesions should be treated with local or systemic therapies according to the location, range or progression rate. In the local control of KS, RT plays an important role. A number of reports showed excellent response rates up to 98.7% after 13.5 years of follow-up [5-7].
Incidence of the KS in South Korea is very low and thus most of the researches were case reports [8,9]. Considering geographic variation of the KS, it would be important to review the treatment in a single-race group. To address this issue, we reviewed single institution experience of RT in treatment of NAKS.
Materials and Methods
The records of the patients who were diagnosed pathologically with KS within the period from February 1998 to January 2012 were retrieved from the archives of the pathologic reports of Seoul National University Hospital in Seoul, South Korea. The protocol approved by the Institutional Review Board. Variables that might affect treatment response such as underlying disease causing immunodeficiency, underlying skin disease, location, numbers of tumor in one irradiation field, field size, radiation dose and fractionation schedule were evaluated. Symptoms at initial presentation (swelling, itching, and pain) were also investigated. Complete response (CR) and partial response (PR) were defined as no clinically detectable tumor and regression of 50% or more in tumor size or fading of the typical color of the lesion, respectively. To assess the correlation between response and variables, logistic regression model was used.
1. Patients characteristics
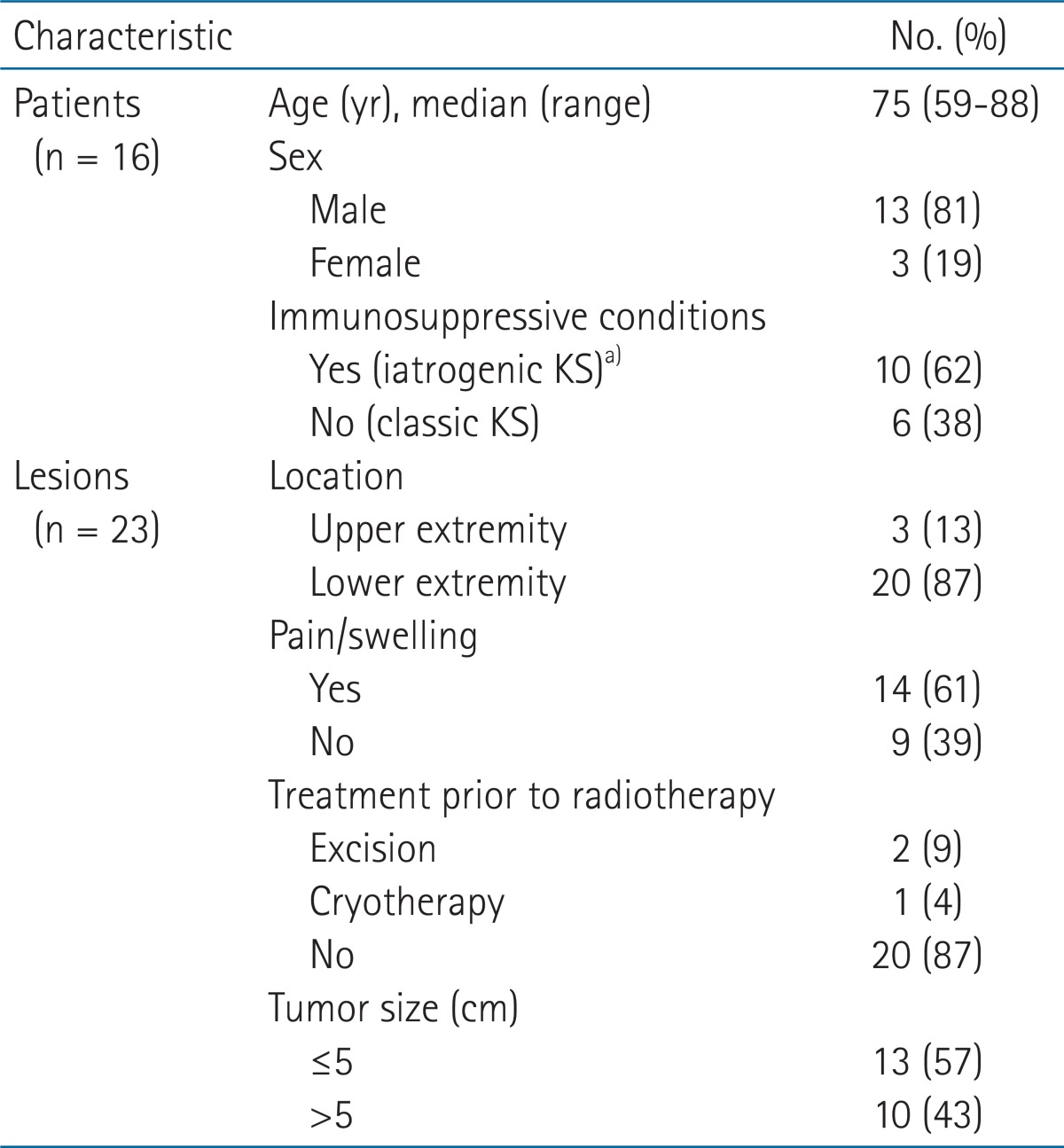
Of 64 patients, 17 received RT at our institution, and had at least one follow-up afterwards. We excluded 1 patient with underlying HIV infection and remaining 16 were included. Of the 16 patients, 13 (81%) were male and 3 (19%) were female. The median age of the patients was 75 years with a range of 59-88 years. To evaluate the response of RT by radiation dose and tumor size, all were divided by treatment field and there were 23 lesions. One lesion had prior trauma history but none of the remainders had underlying skin problem. Detailed information is provided in Table 1.
Three (19%) patients had additional malignancies (two, malignant lymphomas and one, stomach cancer) and underwent chemotherapy before radiotherapy of KS. Including those, 10 (63%) patients had underlying conditions that might cause immunodeficiency: 7 diabetes mellitus (DM), 3 previous chemotherapy (one with DM), and 1 previous kidney transplantation. Therefore, we subcategorized these 10 patients into iatrogenic KS and 6 into classic KS. Other treatment was performed in 3 patients before RT, 2 had excision and 1 had cryotherapy but all had recurrence afterwards demanding additional treatment.
We investigated the KSHV latency-associated nuclear antigen (LANA-1) status but the tests were performed only in 6 patients and all were positive. There was no relationship with KSHV-LANA-1 status and KS subtype.
2. Radiotherapy
Median dose of 36 Gy was given using 1.8-3.0 Gy per fraction, with a range of 24 to 45 Gy. Considering various fractionation schedules, doses were converted into normalized total dose in 2 Gy/fraction (NTD2Gy) and median was 35.4 Gy (range, 26 to 44.3 Gy). Planned target volume was defined as 1.5-2 cm additional margin to the gross tumor volume. Radiation energy was selected by the location and depth of the tumor: 9 (39%) lesions were treated with photon and 14 (61%) with energy electron beam. For the multifocal lesions located on the foot, or the hand, techniques such as bolus application or dipping of the extremities in the water using a small acryl box were used to improve dose homogeneity or reproducibility of alignment (Fig. 1).
Results
1. Treatment response
The median follow-up period was 27.9 months (range, 1.6 to 145.3 months). KS-related or treatment related death was not reported. The follow-up data of remaining 2 lesions in 1 patient were unavailable because the medical records were missing.
Symptom improvement was achieved in 13 (93%) of 14 patients. CR and PR were obtained in 2 (9%) and 19 (73%) lesions, respectively. Fig. 2 shows a case which achieved CR after RT. Two CR lesions remained tumor-free status at the last follow-up (73 and 58 months after RT), but 3 (13%) among the 19 PR lesions underwent local progression at 9.4, 4.4, and 21.5 months after RT, respectively. After local recurrence, 2 received salvage treatment; cryotherapy, imiquimod, and interferon for one, and bleomycin and vincristine for the other.
None of the possible variables (age, sex, symptom at initial presentation, underlying disease, size, or radiation dose) were related with the recurrence. Out-of-field recurrence was reported in 6 patients: 5 patients had recurrence at the same anatomical sites and 1 had at the contralateral site of the primary lesion (left foot to right foot).
Discussion and Conclusion
In AIDS-related KS, highly active antiretroviral therapy (HAART) is the most important, and its response rate was 60% to 90% despite of its systemic and aggressive nature [10,11]. Otherwise, majority of NAKS is indolent and limited to skin therefore mainly locally treatment is enough for either cure or palliation. NAKS contains 3 categories: classic, iatrogenic, and endemic KS [12]. Classic KS is more common in old-aged men, primarily presents at the extremities. Iatrogenic KS is also common in male, and related to immunosuppressive treatment and organ transplantation. Endemic KS affects HIV-seronegative children and young adults in Sub-Saharan Africa. Unlikely with classic and iatrogenic KS, endemic type often contains aggressive nature.
Local treatment modality as, surgical excision, cryotherapy, intralesional vinblastine injection, alitretinoin gel, laser therapy, electrochemotherapy, or RT are used for local control. However, as response evaluation and evaluation timing varies, direct comparison is difficult. In the recent review on classic KS treatment, it was suggested that it was impossible to draw a conclusion for particular intervention due to low qualities of performed studies [2]. Appropriate timing of starting treatment is also a conflicting issue, whether to start at the initial presentation or when symptom occurs. In our institution, we perform treatment when any discomfort or symptom developed, considering indolent behavior.
In our study, 82% of the lesions responded to RT. Considering that medical records of 2 lesions were missing, 100% of lesions with available data showed CR or PR. Three lesions among them progressed locally afterwards, but no correlation was found between possible variables and recurrence. Small number of the cases may partly explain it. Symptom control was achieved in 93% lesions in this study. Although symptom relief was not included as one of the end point by some [2], we believe that symptom control rate as well as size reduction should be comprised of major elements of end results after RT of NAKS. The quality of life after RT is crucial in every patient because pain, itching, or swelling determine activities of the patients, especially in the lesions presented in the lower extremities which enable ambulatory function.
Optimal radiation dose is uncertain. In a study comparing effects of single dose of 6 Gy with 8 Gy, complete response rate was better in 8 Gy group though overall response and progression-free survival were not different [13]. The dose schedule of fractionated RT varied from total dose of 30 Gy in 20 fractions to 35 Gy in 5 fractions. In a retrospective study with 109 KS lesions, RT with lower than rate for NTD2Gy of 20 Gy was related to lower rate of complete response but did not affect overall response rate [14]. In the present study, all the lesions were treated with 26 Gy or higher dose when converted to NTD2Gy. In this range, we could not find the relevance between radiation dose and response. As we achieved sufficient tumor size reduction, symptom relief and acceptable toxicity, these RT dose scheme can be used in this setting effectively. In our study, 6 (38%) of 16 patients were classic KS among NAKS. The classic KS is firstly found in Sub-Saharan Africa or Mediterranean people or their immigrants, but report of classic KS in Asian is very few [15-17] and are mostly from China, Japan or Taiwan, with additional case reports from Korea. Even in the single country, the infection of HHV-8 and incidence of KS varies among races as in Uyghur population [17]. We tried to analyze immunohistochemical status but failed to draw any conclusion because not all the patients had HHV-8 study. In the future, HHV-8 infection rate has to be investigated to evaluate its prognostic value and response parameter for specific treatment.
In conclusion, Local RT achieved 100% response and 93% of symptom relief with acceptable toxicity for this rare, slow-growing, and non-life threatening tumor of non-AIDS associated Kaposi's sarcoma.