Introduction
Colorectal cancers are the third most common cancer in terms of incidence and the second leading cause of death due to cancer worldwide [1]. Out of every ten patients with colorectal cancer, almost four patients have rectal cancer [1]. Treatment of locally advanced rectal cancer (LARC) has evolved over the last 40 years. Currently, the standard treatment of colorectal cancer is neoadjuvant long-course chemoradiation (neo-CRT) followed by total mesorectal excision (TME) surgery after a waiting period of 8–12 weeks [2]. This treatment approach can reduce tumor size and local recurrence and improve patients' overall survival (OS) and disease-free survival (DFS) [3]. Response to neo-CRT is an independent predictor of survival in rectal cancers [4]. After neo-CRT, patients will respond differently [5]. Approximately 15% of patients achieve a pathologic complete response (pCR) in which there will be no viable tumor cells in the resected specimen [5]. Patients with pCR after neo-CRT have better OS and DFS than non-pCR patients [6,7]. We can use organ preservation approaches in pCR patients providing equivalent oncological outcomes with less morbidity and complications [8]. On the other hand, it is rational to resect non-responder patients sooner without having to wait for 8–12 weeks or consider alternative neoadjuvant treatments [9]. Therefore, it will be more beneficial to have the ability to predict the pathologic response rate of patients to neo-CRT with no time wasting.
In the studies conducted in recent years, researchers introduced multiple measurable blood biomarkers as potential predictors of response rate, but so far, no definitive relationship has been found [10-12]. Some of these studies reported meaningful relationship between the lymphocyte-to-monocyte ratio (LMR), carcinoembryonic antigen (CEA), neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR) and pathologic response rate [11] while others did not found any association between these factors and response rate [10] and there are still contradictory results. In the most recent retrospective study, higher LMR was associated with a better response rate; meanwhile, higher NLR and PLR were observed in poor response rate patients [13].
This prospective study investigates the relationship between measurable tumor inflammation-related blood factors (NLR, LMR, total white blood cell count, and PLR) and pathological response rate to new-CRT. The advantage of conducting this study compared to similar previous ones is the prospective design of this study and the use of standard and up-to-date chemoradiation in all eligible patients.
Materials and Methods
1. Patients
In this prospective cohort study, we analyzed patients with LARC who underwent standard neo-CRT and surgical removal of the rectal mass by TME between 2020 and 2022 in a tertiary medical center.
Patients were included in this study if they had all of these criteria: (1) rectal mass adenocarcinoma confirmed with colonoscopic biopsy; (2) confirmed clinical 7th edition of the American Joint Committee on Cancer staging of II/III by endoscopic ultrasonography or magnetic resonance imaging (MRI) with apparent diffusion coefficient/dynamic contrast enhanced protocol; (3) no evidence of metastatic disease in computerized tomography scan; (4) no previous history of pelvic radiotherapy, chemotherapy or target therapy of any kind; (5) no previous or current history of active connective tissue disorders; and (6) no active systemic inflammation. After assessing the patients for mentioned criteria, 34 patients were eligible to be recruited in this study.
This study was performed in line with the principles of the Declaration of Helsinki. The local Institutional Review Board of Baqiyatallah University of medical sciences and the hospital's ethics committee approved the current study (No. IR.BMSU.BAQ.REC.1399.061, date 2021-03-02). Inform consent was obtained from all patients.
2. Treatments
All patients underwent long-course radiotherapy for 25 or 28 fractions of 1.8 Gy/fraction or 2.0 Gy/fraction and 5-fluorouracil (5FU)-based concurrent chemotherapy (capecitabine 825 mg/m2 twice daily throughout the irradiation course). No additional cycle of chemotherapy was administered in the interval between the completion of radiotherapy and surgery. Due to the cardiac side effects of the 5FU-based chemotherapy, cardiac counseling was requested for the patients. Radiotherapy was delivered with the four-field three-dimensional conformal radiation therapy (3DCRT) technique for all of the patients in this study. The treatment field consisted of the primary tumor and high-risk nodes of the pelvic region. Blood samples of patients were evaluated weekly from 1st week to 5th week during chemoradiation with respect to NLR, PLR, monocyte lymphocyte ratio (MLR), and immune inflammation index (SII). Surgery was performed after 8–12 weeks of radiotherapy, and all patients underwent standard TME. All patients received standard 4-month of adjuvant CepeOX (capecitabine and oxaliplatin) or FOLFOX (5FU, leucovorin, and oxaliplatin) chemotherapy based on the National Comprehensive Cancer Network guidelines.
3. Data collection and definitions
Pathologic response to neoadjuvant chemoradiotherapy was reported based on a 3-point tumor regression grade (TRG) system. Based on this scoring system, patients with no viable cancer cells in the primary tumor were defined as TRG0 or pCR. TRG1 was considered as single cells or microscopic residual cancer cells; TRG2 was defined as residual cancer with a desmoplastic response; TRG3 was defined as minimal evidence of tumor response. Patients with TRG0 or TRG1 were grouped as having a good response and patients with TRG2 or TRG3 were grouped as having a poor response. The location of the tumor was defined based on the distance between the anal verge and distal location of the tumor and then categorized into two main groups: lower rectum (less than 6 cm from the anal verge) and higher rectum (more than 6 cm from the anal verge). The inflammatory markers studied in this trial were calculated using mentioned formulas from acquired laboratory data:
NLR ratio: the ratio between 5th week NLR and 1st week NLR;
PLR ratio: the ratio between 5th week PLR and 1st week PLR;
MLR ratio: the ratio between 5th week PLR and 1st week MLR;
SII ratio: the ratio between 5th week SII and 1st week SII.
4. Statistical analysis
Descriptive and frequency analyses were used. The continuous variables are expressed as median with 25th and 75th percentiles. We used Kolmogorov-Smirnov analysis to determine the normality of the quantitative data and it indicated that the data is non-normal. Wilcoxon signed-ranks method was used to assess the changes in pre-defined laboratory parameters and also comparing the laboratory values between two time points. Receiver operating characteristic curve analysis was used to determine the best cut-off points for the pre-defined quantitative laboratory parameters based on the maximum value achieved for the sum of sensitivity and specificity. Logistic regression analysis was also utilized to determine whether any lab parameters during different time point assessments or their relative changes could predict the tumor response based on a permanent pathology review. A p-value less than 0.05 was considered significant for all analyses. All the statistical analyses were conducted using IBM SPSS statistics for Windows, version 26.0 (IBM Corp., Armonk, NY, USA).
Results
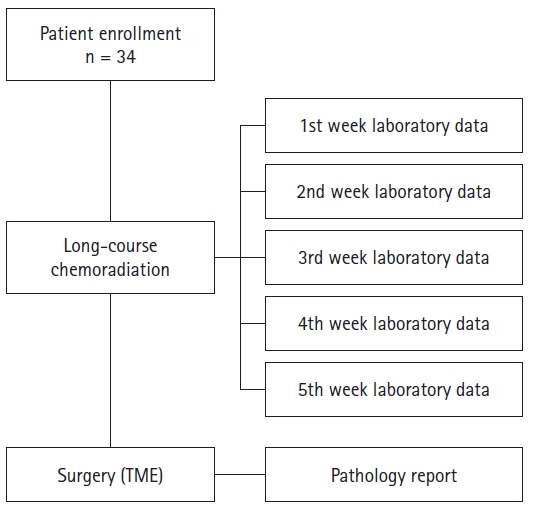
Thirty-four patients with a confirmed diagnosis of LARC were recruited for the study (Fig. 1), including 22 (62.9%) men and a mean ± standard deviation age of 58.9 ± 13.1 years. Table 1 depicts baseline patient and tumor characteristics (tumor stage, tumor location, diabetes, and smoking status).
All patients received 3DCRT to 50–54 Gy with 1.8–2 Gy dose per fraction in 5–5.5 weeks concurrently with capecitabine 825 mg/m2 body square area twice daily during radiotherapy sessions. Patients underwent surgery within 8–12 weeks of the last radiotherapy session.
Eleven patients (32.4%) achieved pCR (TRG0). Seven patients (20.6%) achieved TRG1, whereas 16 patients showed poor response to neoadjuvant treatment according to the pathologic review (13 TRG2 and 3 TRG3).
The patients underwent blood tests weekly during chemoradiation. NLR, PLR, MLR, and SII were calculated for each patient during chemoradiation (Table 2).
Analysis by Wilcoxon signed-ranks method indicated significant rises in NLR, PLR, MLR, and SII on weekly assessments during chemoradiation.
As described before and according to the analysis, having an NLR over 3.21 on the last laboratory test during chemoradiation was correlated with the pathological response on a Pearson chi-squared test (χ2 = 4.2, p = 0.04). Also, a significant correlation was found between the PLR ratio over 1.8 and pathological response (χ2 = 5.25, p = 0.022). NLR ratio over 1.82 marginally missed a significant correlation with the pathological response (χ2 = 2.33, p = 0.13).
Table 3 shows univariate/multivariate regression analysis of the inflammatory markers and pathologic response. As shown on multivariable analysis, a PLR ratio over 1.8 showed a trend for response prediction after controlling for confounders including age, sex, and clinical stage.
Discussion and Conclusion
Based on our findings, of the 34 LARC patients enrolled in this study, 53% had a good pathologic response (TRG0 and TRG1), and 47% had a poor response (TRG2 and TRG3) to neo-CRT treatment. Unlike most of the studies conducted so far, in this study, by performing weekly blood tests during treatment, it was possible to determine the blood cell ratios between different weeks of treatment. Based on the measurements performed in the present study, no correlation was found between the NLR, PLR, MLR, and SII measured based on laboratory tests before the treatment initiation or during the 1st week of radiotherapy and the rate of pathological response. On the other hand, in patients whose measured PLR ratio of the 5th week to the 1st week was more than 1.8, there was a higher clinical response rate to chemoradiation.
The current standard treatment for LARC patients consists of neoadjuvant radiotherapy and concurrent 5FU-based chemotherapy followed by delayed TME surgery [2]. Surgery can be delayed or eliminated in patients who have a good response to neoadjuvant treatment. On the other hand, in patients with poor response to neoadjuvant therapy, a more intensive approach such as total neoadjuvant therapy can be performed. Hence, the possibility of predicting the extent of pathological response to neoadjuvant treatment can significantly affect the treatment approach of patients. MRI and positron emission tomography (PET) scans are currently non-invasive methods for determining clinical response rates [14,15]. Studies have shown that the conduction of PET scan after radiotherapy treatment significantly correlates with the clinical response rate [16,17]. It is worth mentioning that the cost of performing these methods is much higher compared to performing blood sample tests. As response assessment by colonoscopy, MRI or PET is reserved for about 8 weeks after CRT, using inflammatory values and ratios initially and during CRT provides an earlier understanding of the potential capability of the patient to be a responder.
In LARC, the rate of response to treatment is not solely dependent on the initial stage of the disease or the demographic characteristics of the patients, and many factors are influential in determining this response [18]. Additionally, the response occurs heterogeneously in different patients, even those with the same cancer stage [5,10]. So far, several studies have shown a significant relationship between inflammatory factors and the presence of cancers [19]. Also, a shred of evidence has been found in line with the existence of a relationship between these inflammatory factors and the ability to predict the prognosis or treatment response rate of the patients [20-26]. On the other hand, some contradictory and unpredictable correlations between response rate and inflammatory markers have been found in some current studies [27-30]. These controversial findings led us to investigate and assess the possible correlation between inflammatory blood markers in predicting the pathological response after neo-CRT in patients with LARC. Another issue to mention is that the exact mechanism supporting this relationship has not yet been entirely determined [31]. Currently, the biggest concern in using these non-invasive methods is the high probability of error in determining the patients with a complete pathological response.
NLR, PLR, MLR, and SII are the most common inflammatory blood factors studied. In a retrospective study by Wang et al. [13], evaluating 273 LARC, higher pretreatment NLR and PLR (measured based on lab data from 1 week before initiation of chemoradiation) were related to poor pathological response (p = 0.025 and p < 0.0001, respectively). These results were in line with another retrospective study by Li et al. [11], in which pretreatment NLR, PLR, and MLR were significant predictors of pCR. In contrast, in a retrospective study by Zhang et al. [32] conducted in China on 472 LARC, the high-NLR group had lower pCR rates, but the difference was not significant. Likewise, another study showed no significant correlation between pretreatment NLR and PLR with pathologic response rate [10].
In most studies carried out so far, the investigations have been done only on the laboratory tests before the initiation of the radiotherapy. This hypothesis is reasonable to calculate the tumor response rate to radiotherapy by comparing the laboratory tests done after the radiation with the tests before the chemoradiation initiation at different time levels. As far as we know, the study by Lee et al. [33] in Korea was the only study that evaluated the patients' laboratory tests at different time intervals during radiotherapy. In their retrospective study, patients' laboratory tests were collected and analyzed at three stages; before chemoradiation, 3 weeks after the chemoradiation initiation, and 4 weeks after chemoradiation completion. Also, the changes in these values were investigated in different stages. Lee et al. [33] found a significant correlation between low pretherapy NLR, high intratherapy NLR and PLR, high intratherapy NLR ratio (intratherapy NLR divided by pretherapy NLR), and PLR ratio (intratherapy PLR divided by pretherapy PLR) with pathological complete response.
In the current study, blood samples of patients were examined weekly during radiotherapy treatment, and inflammatory markers such as NLR, PLR, MLR, and SII were calculated from these samples. Also, instead of analyzing a single pretreatment laboratory value for determining its correlation with the eventually achieved response, we investigated whether there was any correlation between the velocity of temporal changes in the mentioned values and the response. In a univariate analysis, our results showed that patients achieving a PLR on the 5th week of radiotherapy over 1.8 times the initial PLR (PLR ratio) are 6.6 times more likely to reach a complete or near-complete response on the permanent pathology. Moreover, this PLR ratio kept its significance on a multivariable analysis after considering the effect of confounders including age, sex, and initial clinical stage.
To our knowledge, this is the first prospective cohort that examined the weekly blood samples of patients during chemoradiation. In addition, due to the shorter sequence between samplings, it was possible to determine the details of changes in inflammatory factors during the course of radiotherapy for the first time. According to previous studies, chemotherapy in the interval between the completion of radiotherapy and surgery has increased the pathological response rate; therefore, patients who received chemotherapy outside the course of radiotherapy were not included in the study [34,35]. Likewise, the radiation treatment method and dose were common among patients. In addition, it is suggested that associated pathways and related genes be considered intelligent targets for treating rectal cancers at the molecular levels [36].
Several limitations need to be addressed in this study. First, the number of patients evaluated in this study was relatively small, and by increasing the number of patients examined, more robust results could probably be obtained. Second, to eliminate the interobserver error in determining the response rate, it would be better to review all pathology samples by a single pathologist.
In conclusion, our study showed that the magnitude of change in inflammatory markers, especially platelet to lymphocyte ratio, through the neo-CRT course can have a borderline effect on the prediction of complete/near-complete pathological response on the permanent pathology.