Introduction
Recent improvements in radiation therapy (RT) techniques as well as knowledge on radiobiological consideration in liver RT have enabled us to deliver enough dose of radiation to get a substantial local control of hepatocellular carcinoma (HCC) [123456]. Though the scientific evidences of multidisciplinary approach combined with radiation are lacking, RT has been tried frequently as a combined modality for treating naïve HCC patients especially in Asia-Pacific countries [7810]. RT has also been tried as a salvage treatment in patients with recurrent HCC which is refractory to or ineligible for other therapies, and showed excellent local control with favorable survival outcomes [111213].
In the clinical reality, we face the situations that re-irradiation is needed for the patients with recurrent HCC, mainly due to the lack of available local salvage modalities for the very patients [14]. The biological properties of liver regeneration as a parallel organ have been studied primarily in surgical settings following partial hepatectomy, but several studies also showed unirradiated liver regions regenerating after proton radiation and stereotactic body RT [151617]. Additionally, there have been recent experimental animal studies demonstrating the regeneration kinetics of hepatic proliferation after liver irradiation [1819]. Hepatic re-irradiation in patients with HCC are being applied based on such theoretical basis and increasing needs in the clinic, but studies on re-irradiation have been seldom reported.
In this study, we evaluated the efficacy and toxicity of repeated high-dose 3-dimensional conformal RT (3D-CRT) for patients with recurrent HCC, and also investigated the factors affecting the treatment outcomes.
Materials and Methods
This study was approved and exempted from the permission requirement by the Institutional Review Board of Samsung Medical Center (IRB No. 2013-09-078).
1. Patients
From 1998 to 2011, 45 patients with unresectable HCC received liver directed second RT with high dose 3D-CRT in Samsung Medical Center. The eligibility criteria for repeated RT were as follows: 1) HCC not eligible for or refractory to other therapies; 2) persistent disease after initial RT. We included 43 patients by excluding two ineligible patients, one with immediate follow-up loss and the other who underwent liver transplantation after second RT. Radiation-related and medical records of the eligible patients were retrospectively reviewed.
2. Radiation therapy
Computed tomography (CT) scans for RT planning were done with each patient in a supine position, with both arms raised above the head. CT simulation data were transferred to a 3D-CRT planning system (from 1998 to 2003, PROWESS, Alliant Medical Technology, Chico, CA, USA; from 2004 to 2011, PINNACLE, The Philips Medical System, Madison, WI, USA). The tumor, normal liver, kidneys, spinal cord, and bowels were contoured and reconstructed to form a 3-demensional representation.
The clinical target volume (CTV) was regarded same as the gross tumor volume. To determine the cranial-caudal margins, the diaphragmatic excursion during respiration was visualized using fluoroscope, and CTV was expanded by the amplitude of this excursion (1.5-2.5 cm). RT was delivered with a 6- to 15-MV linear accelerator. Treatment planning for re-irradiation was performed with an emphasis on maximizing non-irradiated liver volume and minimizing the overlapped volume of irradiation in the skin using 3D-CRT technique. Total dose was designed under tentative guidelines so that the normal liver volume irradiated with over half of the prescribed dose should not exceed 50% of the total liver volume. The total dose was determined by considering the doses of the remnant functioning liver, gastro-duodenum, and large bowel by the discretion of the treating physician considering previous radiation dose to the critical structures, interval from the previous course of radiotherapy. The re-irradiation dose ranged from 30 to 55 Gy (median, 45 Gy) in daily 2 to 15 Gy (median, 3 Gy) fractions.
3. Follow-up
Tumor response was evaluated on serial CT scans 4 to 6 weeks after completion of second RT and then at 3 months intervals. Tumor response was determined using the criteria from the modified Response Evaluation Criteria in Solid Tumors for HCC [20] based on the reports of the diagnostic radiologists. Survival was calculated from the date that second RT has started.
4. Evaluation of radiation toxicity
Physical examinations and chemistry profiles including liver function were checked on every follow-up visit. Toxicities were assessed using the Common Terminology Criteria for Adverse Events (CTCAE) ver. 4.0. Radiation-induced liver disease (RILD) was separated into 'classic' and 'non-classic' RILD. Classic RILD was characterized by the presence of anicteric ascites and the elevation of alkaline phosphatase levels to at least a 2-fold increase over pretreatment values in the absence of tumor progression. Non-classic RILD was defined as the elevation of liver transaminases more than five times the upper limit of normal or CTCAE grade 4 levels in patients with baseline values more than five times the upper limit of normal within 3 months after completion of RT, or a decline in liver function (measured by worsening of the Child-Pugh score by 2 or more) [2122].
5. Statistics
Tumor response according to RT dose was compared using the chi-square test. Survival was estimated using the Kaplan-Meier method and compared using the log-rank test to determine potential prognosticators. The Cox proportional hazard regression analysis was used for multivariate analysis. A p-value <0.05 was considered to be statistically significant. All aforementioned analyses were performed using IBM SPSS Statistics ver. 20 (IBM, Armonk, NY, USA).
Results
1. Patient characteristics and treatment
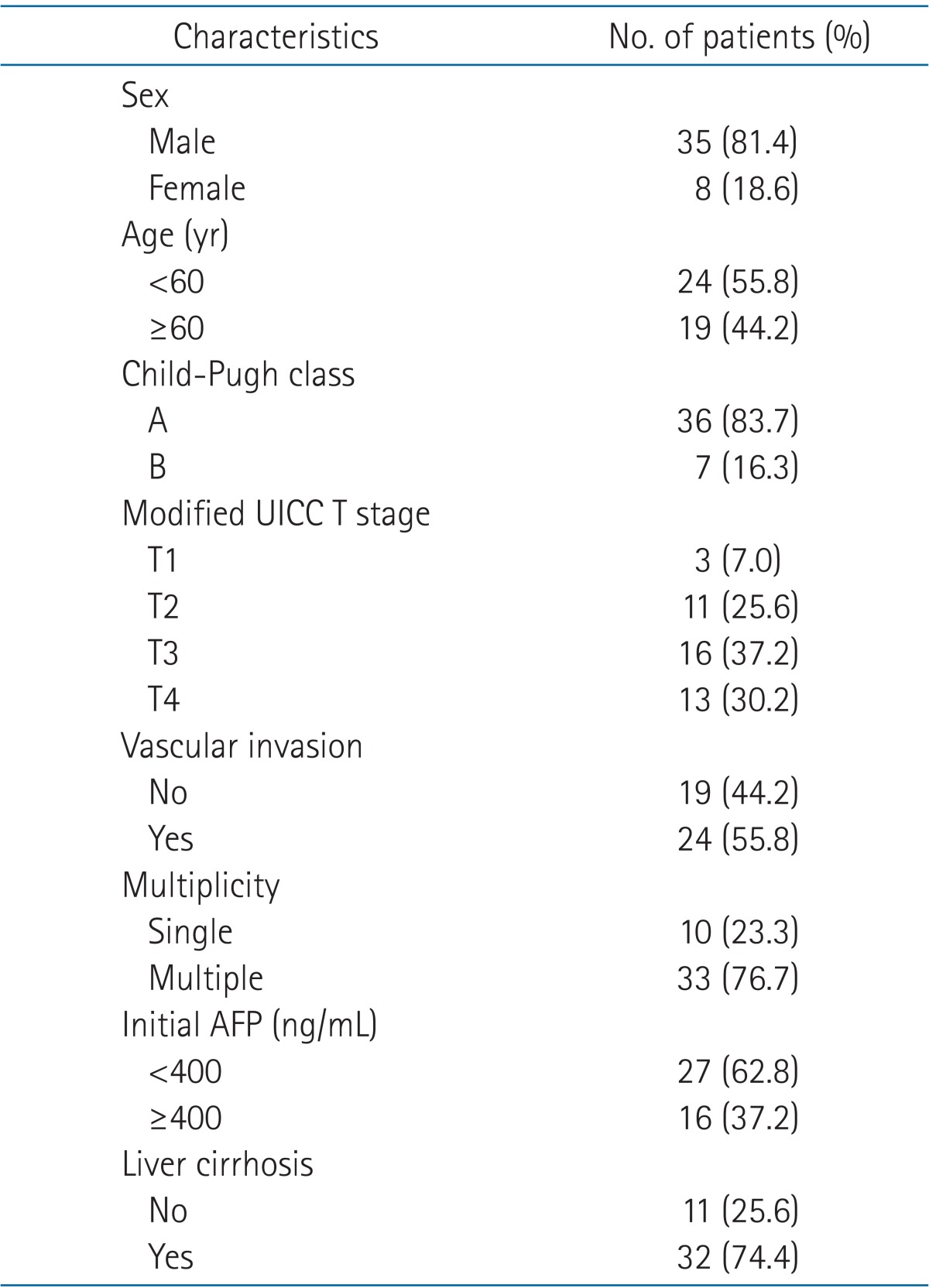
Patient characteristics at the time of second RT are summarized in Table 1. The median age of all patients was 59 years (range, 29 to 71 years). Modified Union for International Cancer Control (UICC) T stage was determined based on the viable tumor evaluated before starting the second RT, and the group of 43 patients was comprised of 30 (69.8%) T1-T3 and 13 (30.2%) T4 patients. Vascular invasion was accompanied in 24 patients (55.8%) and 33 patients (76.7%) had multiple tumors. Majority of patients had a clinical liver function of Child-Pugh A classification (83.7%).
Median interval between first and second RT was 13.8 months (range, 1.0 to 58.1 months). Because different doses per fraction were used, the equivalent doses to 2 Gy fractions (EQD2Gy) for α/β ratio of 10 were calculated. The dose of first RT ranged from 32.5 Gy10 to 93.8 Gy10 (median, 48.8 Gy10). Second RT was delivered with palliative (n = 24) or salvage (n = 19) intent, and the RT dose ranged from 31.25 Gy10 to 93.75 Gy10 (median, 44 Gy10).
Target volumes of second RT in the liver were overlapped with the first RT site in 13 patients (30.2%), adjacent with the volume of first RT in 21 patients (48.8%), and apart from the first RT site in 9 patients (20.9%). Cumulative RT dose in the overlapping target volume from two RT sessions ranged from 65.0 Gy10 to 117.0 Gy10 (median, 90.6 Gy10). Gastro-duodenum was re-exposed in 16 patients (37.2%).
During the follow-up after second RT, additional transarterial chemoembolization (TACE) was performed in 11 patients, radiofrequency ablation in one patient, third RT in three patients, and fourth RT in one patient.
2. Radiographic in-field tumor response rates
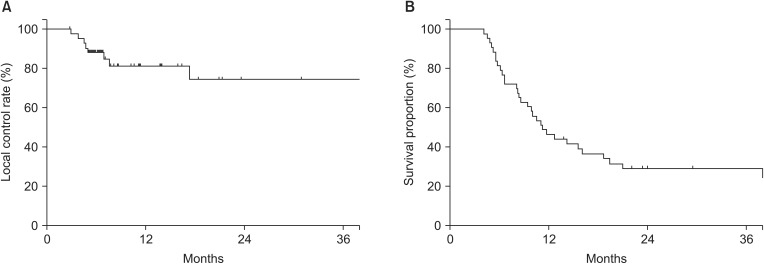
The radiographic in-field tumor responses were evaluable in all patients. An objective tumor response rate was 62.8% with complete response in 8 lesions (18.6%) and partial response in 19 (44.2%). The tumor response rates were 81.0% and 45.5% in patients receiving ≥45 Gy10 and <45 Gy10, respectively (p = 0.016) (Table 2). Local control rate was 84.0% at 1-year and 77.6% at 2-year (Fig. 1A).
3. Survival analysis and predictors of survival
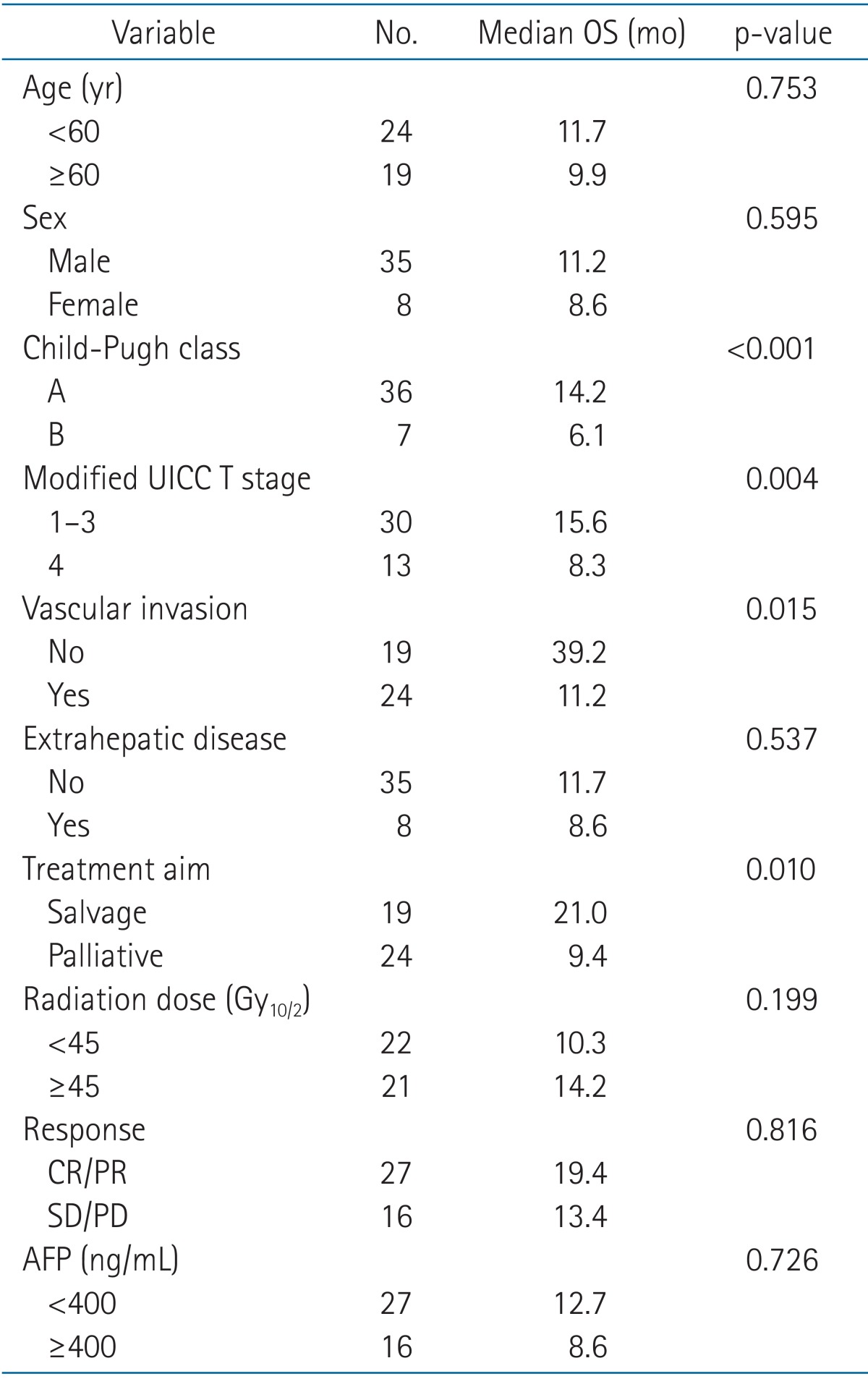
The median follow-up duration calculated from the initiation of the second RT was 11.2 months (range, 4.1 to 58.3 months). During the follow-up period, eight patients remained alive and 35 died. The overall survival (OS) rates at 1- and 2-year were 57% and 38%, respectively (Fig. 1B). The median OS was 11.2 months, and it was significantly affected by the Child-Pugh class and the modified UICC T stage. The median OS were 14.2 months vs. 6.1 months (Child-Pugh A vs. B, p < 0.001) (Fig. 2A) and 15.6 months vs. 8.3 months (T1-3 vs. T4, p = 0.004) (Fig. 2B), respectively (Table 3). Higher RT dose (≥45 Gy10) tended to be associated with better OS (14.2 months vs. 10.3 months, p = 0.199) (Fig. 2C). Median OS increased to 24 months when patients with poor prognostic factor (Child-Pugh Class B and modified UICC T-stage T4) were excluded (Fig. 2D). Overlap of RT volumes in the liver or gastro-duodenum between first and second RT was not significantly related to OS.
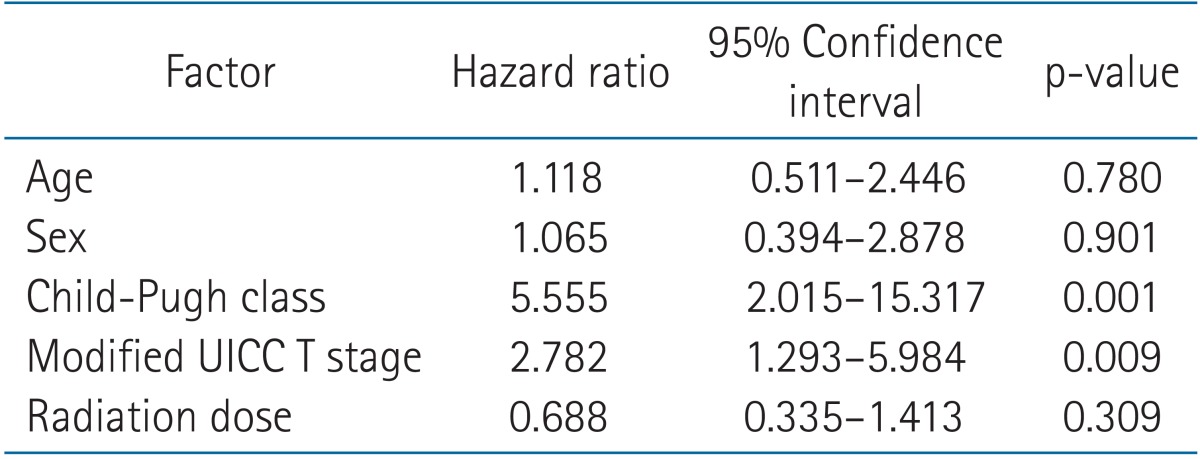
By multivariate analysis (Table 4), the Child-Pugh class and the modified UICC T stage were significant prognostic factors affecting OS (p = 0.001 and p = 0.009, respectively).
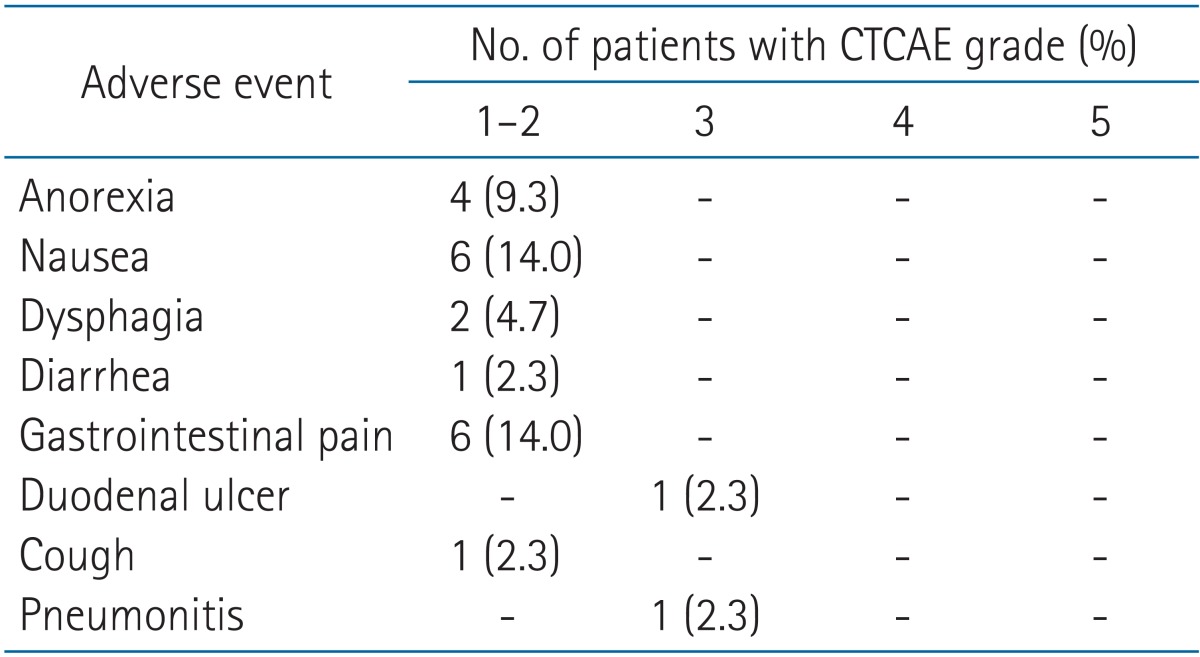
4. Treatment-related toxicities
The profiles of treatment-related RT toxicity are displayed in Table 5. Overall CTCAE grade 1 or 2 toxicities were developed in 18 patients (41.9%). Nausea, anorexia, and gastrointestinal pain were the most common toxicities, but the acute symptoms were resolved spontaneously or with supportive care. Two patients developed grade 3 or higher toxicity during follow-up period, both of them received ≥50 Gy10 at the time of second RT. One patient suffered from grade 3 duodenal perforation and the other from grade 3 pneumonitis. The patient with grade 3 duodenal perforation underwent three times of RT before the adverse event with 45 Gy in 15 fractions and 11 months after the first course with 54 Gy in 18 fractions followed by 48 Gy in 16 fractions after 6 months after the second course. The site of perforation seemed to correlate with the site repetitively exposed with 3 times of RT. Although it was difficult to differentiate RILD from deteriorating liver function associated with disease progression or the side effect of TACE, no definitive classic or non-classic RILD was observed during the follow-up period.
Discussion and Conclusion
In currently available management guidelines for HCC, individual modalities such as sorafenib or TACE are suggested as a sole treatment for unresectable HCC [23]. However, in practice, the orchestration of multimodality treatments is needed for successful treatment of individual patients [8]. Usually the HCC management guidelines suggest initial therapy only at diagnosis. However, since the progression after initial therapy is also an important issue, appropriate salvage treatments should also be recommended [8]. Due to the successful combined treatments for unresectable HCC patients, more patients are getting to outlive the duration of expected benefits from initial palliative RT, and require second session of liver-directed RT for intrahepatic recurrence which is refractory to or ineligible for other loco-regional therapies.
In the liver-directed re-irradiation, special cautions are required as HCC patients tend to have poorer liver function and cirrhosis after repeated liver-directed therapies [46]. Furthermore, re-irradiation to the close proximity with adjacent radiosensitive organs such as stomach and duodenum might cause serious treatment toxicity and its resultant treatment-related death [52425]. Hepatic re-irradiation in patients with HCC has not been studied with an exception of proton re-irradiation [14]. The present study evaluates efficacy, toxicity, and the factors which affect survival rate of hepatic re-irradiation in patients with unresectable HCC.
We compared the treatment outcomes of patients who received ≥45 Gy10 to that of patients who received <45 Gy10 because the tolerance radiation dose of gastrointestinal tract is generally considered to be approximately 45 Gy10 [26]. In the current study, the dose-response relationship existed with statistical significance. The tumor response rates were 81.0% and 45.5% in patients receiving ≥45 Gy10 and <45 Gy10, respectively. It suggests that dose-response relationship in HCC identified by former studies may also be applied to re-irradiation situation [272829]. Survival showed positive relationship with RT dose as well, but with no statistical significance. The group with high dose RT (≥45 Gy10) showed higher median OS of 14.2 months compared to 10.3 months for low dose RT. Statistical significance might be achieved in the future trials using larger sample size.
There were two prognostic factors predicting survival in our analysis: Child-Pugh class and the modified UICC T-stage. While the median OS was 11.2 months, the results showed that it was significantly affected by these two factors. The median OS increased to 24 months when the patients with both Child-Pugh Class B and modified UICC T-stage T4 were excluded (Fig. 2D). This survival figure is close to the formerly reported median OS of first RT as a combined modality on HCC patients [79102930], and it could indicate that re-irradiation can be effective in selected group of patients with Child-Pugh A and T1-3 stage. The other potential prognosticators need further investigation through future studies.
In the toxicity analysis, which is one of most important concerns in re-irradiation situation, two patients developed grade 3 or higher toxicity during follow-up period, both of them received ≥50 Gy10 at the time of second RT. Special caution is required in cases of second RT dose is higher than 50 Gy10 to preserve adjacent gastro-duodenum and reduce the risk of radiation pneumonitis. Although the overlapping of the target volume in the liver or gastro-duodenum did not influence the survival statistics, the grade 3 duodenal perforation developed in a patient who received three times of radiation exposure to the gastro-duodenum. Therefore, specific caution is required in the re-exposure of gastro-duodenum and further studies are needed to reveal the relationship between the dose volumetric parameters after re-irradiation and the development of serious complications.
On the other hand, low complication rate (2 out of 43 patients) may imply that re-irradiation is feasible for selected HCC patients. Treatment result in the current study suggests that re-irradiation can be delivered safely with careful consideration to adjacent organs, even when the treatment field of second RT overlaps with the first RT field in the liver or gastro-duodenum. Considering the current development of RT techniques in precision and accuracy, re-irradiation is expected to be applied more frequently as an option for salvage or palliation.
Limitations of this study include retrospective approach, heterogeneous characteristics of patient group, small sample size and not being able to utilize composite plans to evaluate dose-volume histogram parameters and toxicity. The findings of this study regarding the efficacy and low complication rate of re-irradiation on HCC patients can provide useful data and essential perspective for future prospective studies, but the result is not yet conclusive. It can only suggest a tentative guideline for hepatic re-irradiation and should be further improved by prospective studies with large sample size to establish treatment guidelines and dose constraints for these treatments.
In conclusion, the hepatic re-irradiation for HCC patients may be feasible and tolerable option. It was effective in selected group of patients with Child-Pugh A classification and modified UICC T1-3 stage, and the toxicities were manageable except in two patients who had grade 3 complications. However, to define the role and indication of hepatic re-irradiation in HCC patients, further prospective studies with larger study population are warranted.